
Susun Bellew, DO; James Q. Del Rosso, DO, FAOCD
Valley Hospital Medical Center, Las Vegas, Nevada
Disclosure: Dr. Bellew reports no relevant conflicts of interest. Dr. Del Rosso is a consultant, speaker, and or researcher for Allergan, Coria, Galderma, Graceway, Intendis, Medicis, Onset Therapeutics, Ortho Dermatology, PharmaDerm, Promius, Quinnova, Ranbaxy, SkinMedica, Stiefel, Triax, Unilever, and Warner Chilcott.
Abstract
Ichthyosis vulgaris is an inherited disorder of keratinization that results in asteatotic scales on extensor surfaces of the arm, legs, and trunk. A combination-therapy approach with a physiological lipid-based barrier repair topical emulsion and ammonium lactate 12% lotion applied topically was shown to be effective at four-week follow up without any untoward side effects. This combination therapy addresses the importance of caring for both the corneocytes (“bricks”) and the intercellular lipid bilayer (“mortar”) for optimal benefit. (J Clin Aesthetic Dermatol. 2010;3(7):49–53.)
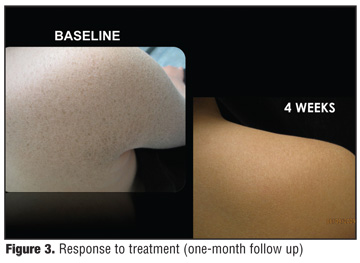
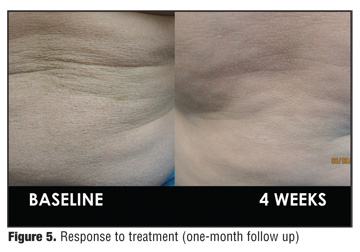
A 10-year-old boy presented with a long-standing history of very dry skin involving the arms, legs, and trunk (Figure 1 and Figure 2). Prior treatment regimens for the current condition were limited to use of over-the-counter moisturizers with limited success. The patient was in general good health with no known drug allergies and was using no medications. Family history was noncontributory except for his mother and one sibling having dry skin. Physical examination exhibited dry, fine, scaly patches on the trunk (Figure 1) and both the upper and lower extremities (Figure 2) with sparing of the flexural surfaces, including the popliteal, antecubital, axillary, and inguinal regions. A diagnosis of ichthyosis vulgaris (IV) was rendered based on the clinical features and history. The patient was treated with a combination regimen including ammonium lactate (AL) 12% lotion (Lac-Hydrin 12% Lotion, Ranbaxy Laboratories, Jacksonville, Florida), followed by a physiological lipid-based barrier repair cream (Ec) containing ceramides, cholesterol, and free fatty acids in a 3:1:1 ratio designed to simulate the normal intercellular lipid bilayer (EpiCeram® Skin Barrier Emulsion, Promius Pharma LLC, Bridgewater, New Jersey). Both formulations were applied sequentially twice daily diffusely to the skin including the affected areas. At the one-month follow-up visit, the patient had essentially complete resolution of ichthyotic scaling and xerosis (Figure 3, Figure 4, Figure 5). The patient remained clear with continued use of the ensuing weeks and was subsequently lost to follow up.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
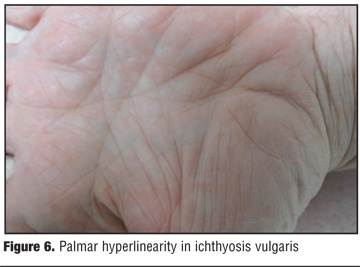
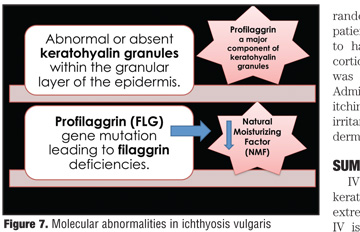
IV is an autosomal semidominant disorder characterized by visible scaling and dryness with noticeable sparing of the flexural surfaces along with palmar and plantar hyperlinearity (Figure 6).[1–3] The term semidominant refers to heterozygous individuals having a milder phenotypic form of the disease with incomplete penetrance as opposed to homozygotes who have a more severe manifestation.[1,3] Individuals with IV have frequent nonsense mutations in the filaggrin gene (FLG), which alters the expression of profilaggrin, a high-molecular weight filaggrin precursor.[3] Profilaggrin is housed in the granular layer of the epidermis by keratohyalin granules, which are reduced in number or completely absent in patients with IV (Figure 7).[3–5]
{kind=link}
{kind=link}
Subsequently, these alterations lead to reflexive epidermal hyperplasia, “clumping” of corneocytes, and abnormal desquamation resulting in the clinical manifestation of scaling.[6]
The role of filaggrin in the differentiation of the epidermis as well as in the maintenance of epidermal barrier function is a crucial one. Upon terminal differentiation, profilaggrin is proteolytically cleaved into multiple filaggrin peptides that aggregate keratin filaments, thus the name filaggrin or filament aggregating protein.[3,4] In many patients with IV, there is concurrent association with atopic dermatitis (AD).[7,8] In fact, studies show that FLG mutations found in IV are also strongly associated with atopic dermatitis and secondary allergic diseases.[7]
“MAJOR PLAYERS” OF THE STRATUM CORNEUM
Our understanding of the complexity of the stratum corneum (SC) has come a long way from the SC being considered an inactive “plastic film.” Advances in benchtop research have led to our recognition that the SC is a structurally and biochemically dynamic entity essential to maintaining the homeostatic function of the epidermal skin barrier.[9] In healthy skin, the SC is essentially an impermeable membrane to the environment. It only allows for small amounts of physiological transepidermal water loss (TEWL), enough to maintain hydration of the corneal layer. Adequate SC hydration is needed to maintain skin for flexibility with avoidance of microfissuring, to catalyze hydrolytic enzyme activity involved in normal corneocyte maturation and physiological desquamation, and desmolysis allowing for shedding of individual corneocytes.10 To simplify this highly specialized structure, the SC has been compared to a brick wall consisting of protein-enriched corneocytes or terminally differentiated keratinocytes (bricks) enveloped by a surrounding intercellular lipid bilayer membrane (mortar).[11] The corneocytes are “spot-welded” by corneodesmosomes at several points and stacked on top of one another.[12]
The corneocyte bricks constitute a scaffold framework around which the intercellular lipid bilayer is able to wrap itself in a continuous fashion.[6] The intercellular lipid bilayer also provides a tortuous pathway preventing excessive TEWL and acts as a physical barrier for environmental stresses.[6] Corneocytes mainly consist of protein-rich keratin filaments encapsulated within a protein/lipid polymer structure, referred to as the cornified cell envelope (CE).[13] The lipid component of the CE interacts directly with the lipid-rich intercellular mortar.[13]
Another important player in maintaining epidermal barrier integrity and function is natural moisturizing factor (NMF) found within corneocytes. NMF, which is derived from filaggrin, comprises a mixture of amino acids, lactic acid, urea, citrate, sugar, and inorganic ions, and functions to serve as the inherent humectant of the epidermis (“nature’s humectants”).[14] Mechanistically, NMF absorbs atmospheric water and retains necessary hydration that is vital for proper functioning and turnover of the SC.[15] NMF is produced by proteolysis of filaggrin during corneocyte maturation, and its release is tightly regulated by environmental humidity as well as the filaggrin/keratin complex.[15] This complex is resistant to proteolysis and ultimately prevents premature degradation of filaggrin.[15]
The intercellular lipid bilayer (mortar) has the arduous task of acting as the permeability barrier of the skin consisting mainly of ceramides (approximately 50% by mass), cholesterol (25%), and free fatty acids (10–20%) (Figure 8).[16–18] This ratio is crucial as deficiencies in any of the intercellular lipid components can result in epidermal barrier dysfunction, characterized by an increase in TEWL, subsequent impairment of physiological desquamation with development of scaling, and reduced skin plasticity leading to micro- and macrofissuring of the skin.[12] The majority of lipids are derived from lamellar bodies (LBs) in the stratum granulosum layer of the epidermis.[10] During terminal differentiation, LBs bud off in a trans-Golgi-like network and secrete their precursor lipid contents into the interface of the stratum granulosum and the SC where they are cleaved by co-secreted enzymes to generate ceramide-dominant lipid membrane structures.[19] These lipids then bind to form the intercellular lipid bilayer membrane, referred to as the mortar, of the SC.
{kind=link}
RATIONALE FOR COMBINATION TREATMENT FOR ICHTHYOSIS VULGARIS
There is limited information available regarding effective therapies for IV. Most conventional treatment regimens for IV, and even for xerosis, focus on either the bricks or the mortar components of the SC. A limitation of this approach is failure to address the functional interdependence of both the brick and mortar components. It seems more prudent to incorporate therapy aimed at treating both components of the epidermal barrier, that is the corneocytes and the intercellular lipid bilayer membrane. The current case illustrates the combined use of AL 12% lotion and Ec cream which resulted in resolution of IV.
Much of the evidence supporting the combination topical therapy approach selected for treatment of this patient is derived from research in patients with AD who also have similar FLG mutations leading to filaggrin deficiencies. Although inflammation is not inevitable or generally visible clinically in IV, the common association of AD and IV in the same individuals is both a clinical and biological link. The most immediate response to deficiencies in filaggrin as seen in patients with IV and AD is decreased corneocyte hydration.[20] To this end, the ability of AL to enhance SC hydration in the treatment of IV has been extensively studied.[21–24] AL is lactic acid (an alpha-hydroxy acid) buffered with ammonium hydroxide to provide a pH of 4.4 to 5.5.[25] As mentioned earlier, lactic acid was identified as one of the major constituents of NMF, and thus is used as moisturization therapy for xerotic skin conditions.[22]
Further studies found that AL has additional properties beyond its role as a humectant. In-vivo studies indicate that the L-isomer of lactic acid stimulates ceramide biosynthesis, thus treating the mortar component by enhancing the intercellular lipid bilayer.[26] Furthermore, topical AL was shown to reduce cutaneous atrophy induced by application of potent topical corticosteroids, with AL counteracting both the epidermal thinning and the decrease in dermal matrix seen with continued corticosteroid use.[27] It has been illustrated that a topical AL 2 to 10% solution increased dermal glycosaminoglycans.[24] Moreover, a study that compared AL 5%, AL 12%, and a nonlactate emollient showed that patients who applied AL 12% lotion exhibited a slower relapse of xerotic skin changes during the regression period after treatment was discontinued.[28]
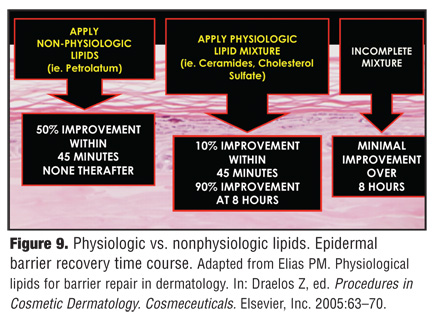
When stratum corneum barrier integrity is disrupted, a repair sequence is rapidly initiated to reinstate homeostasis.[29] Studies have shown that application of complete physiological lipid mixtures containing ceramides, cholesterol, and fatty acids in the proper ratio facilitates the barrier recovery mechanism. In contrast, key lipids applied individually, and not as a physiologically rational mixture, can actually prolong the barrier repair process.[30] Physiological lipid mixtures, such as Ec cream, traverse the epidermis and the individual lipid components may be incorporated into lamellar bodies at the granular layer after application. Nonphysiological occlusive agents (i.e., petrolatum ointment) remain localized and primarily restricted to the superficial stratum corneum.[31]
As a result, an occlusive agent, such as petrolatum, may create a rapid decrease in TEWL; however, a sustained effect on barrier repair is limited. On the contrary, a physiological lipid mixture, such as Ec cream, may be slower in onset; however, the therapeutic impact on barrier repair and recovery is greater in benefit and of more sustained duration than an occlusive agent or nonphysiological lipid formulation (Figure 9).
{kind=link}
Ec cream is a ceramide dominant barrier repair cream containing all three key lipids (ceramide, cholesterol, free fatty acids) in an optimized 3:1:1 molar ratio, thereby increasing the lipid bilayer and ultimately treating the mortar component of the barrier.[32,33] In a multicenter, randomized, investigator-blinded, clinical trial of 121 patients with moderate-to-severe AD, Ec cream was found to have comparable efficacy to a mid-strength topical corticosteroid with a favorable safety profile.[33] Ec cream was approved by the United States Food and Drug Administration in April 2006 for treatment of burning and itching associated with dry skin conditions, such as AD, irritant contact dermatitis, radiation dermatitis, and other dermatoses.[34]
SUMMARY
IV is an autosomal semidominant inherited disorder of keratinization characterized by dry, fine scales on the extremities and trunk with sparing of the flexural surfaces. IV is associated with FLG mutation leading to altered profilaggrin production and subsequent decreases in filaggrin. Treatment should be directed toward caring for both bricks and mortar components of the stratum corneum. The combination therapy of Ec and AL 12% lotion addresses both elements in order to optimize treatment for the IV patient.
References
1. Oji V, Traupe H. Ichthyosis. Clinical manifestations and practical treatment options. Am J Clin Dermatol. 2009;10(6):351–364.
2. Akiyama M, Shimizu H. An update on molecular aspects of the non-syndromic ichthyoses. Exp Dermatol. 2008;17: 373–382.
3. Smith FJ, Irvine AD, Terron-Kwiatkowski, et al. Loss-of-function mutations in the gene encoding filaggrin cause ichthyosis vulgaris. Nat Genet. 2006;38:337–342.
4. McGrath J. Filaggrin and the great epidermal barrier grief. Australas J Dermatol. 2008;49(2):67–73.
5. Sybert VP, Dale BA, Holbrook KA. Ichthyosis vulgaris: identification of a defect in synthesis of filaggrin correlated with an absence of keratohyaline granules. J Invest Dermatol. 1985;84:191–194.
6. Schmuth M, Gruber R, Elias P. Ichthyosis update: towards a function-driven model of pathogenesis of the disorders of cornification and the role of corneocyte proteins in these disorders. Adv Dermatol. 2007;23:231–256.
7. Palmer CN, Irvine AD, Terron-Kwiatkowski A, et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet. 2006;38:44–46.
8. Sandilands A, Terron-Kwiatkowski A, Hull PR, et al. Comprehensive analysis of the gene encoding filaggrin uncovers prevalent and rare mutations in ichthyosis vulagris and atopic eczema. Nat Genet. 2007;39(5):650–654.
9. Scleuplein RJ, Blank IH. Permeability of the skin. Phsiol Rev. 1971;51(4):702–747.
10. Harding CR, Watkinson A, Rawlings AV. Dry skin, moisturization and corneodesmolysis. Int J Cosmet Sci. 2000;22:21–52.
11. Elias PM. Epidermal lipids, barrier function and desquamation. J Invest Dermatol. 1983;80(suppl 1):44–49.
12. Menon GK, Norlen L. Stratum corneum ceramides and their role in skin barrier function. In: Leyden J, Rawlings A, eds. Skin Moisturization. New York: Marcel Dekker Inc.; 2002:40–55.
13. Nemes Z, Steinert PM. Bricks and mortar of the epidermal barrier. Exp Mol Med. 1999;31(1):5–19.
14. Cler EJ, Fourtanier A. L’acide pyrrolidone carboxylique (PCA) et la peau. Int J Cosmet Sci. 1981;3:101–113.
15. Rawlings AV, Harding CR. Moisturization and skin barrier function. Dermatol Ther. 2004;17 (suppl 1):43–48.
16. Bouwstra JA, Dubbelaar FER, Gooris GS, et al. The role of ceramide composition in the lipid organization of the skin barrier. Biochim Biophys Acta. 1999;1419:127–136.
17. Norlen L, Nicander I, Lundh-Rozell B, et al. Inter and intra individual differences in stratum corneum lipid content related to physical parameters of skin barrier function in-vivo. J Invest Dermatol. 1999;112:72–77.
18. Wertz PW, van den Bergh B. The physical, chemical and functional properties of lipids in the skin and other biological barriers. Chem Phys Lipids. 1998;91:85–96.
19. Elias PM, Cullander C, Mauro T, et al. The secretory granular cell: the outermost granular cell as a specialized secretory cell. J Invest Dermatol Symp Oroc. 1998;3:87–100.
20. Elias PM. Barrier repair trumps immunology in the pathogenesis and therapy of atopic dermatitis. Drug Discov Today Dis Mech. 2008;5(1):e33–e38.
21. Van Scott EJ, Yu RJ. Control of keratinization with a-hydroxy acids and related compounds. Arch Dermtol. 1974;110: 586–590.
22. Middleton JD. Development of a skin cream designed to reduce dry and flaky skin. J Soc Cosmet Chem. 1974;25:519–534.
23. Alderson SG, Barratt MD, Black JG. Effect of 2-hydroxyacids on guinea-pig footpad statum corneum: mechanical properties and binding studies. Int J Cosm Sci. 1984;6:91–100.
24. Leyden JJ, Lavker RM, Grove G, et al. Alpha hydroxyl acids are more than moisturizers. J Geriatr Dermatol. 1995;3(suppl):33A–37A.
25. Lac-Hydrin (Ammonium Lactate) Lotion [package insert]. Princeton, NJ: Ranbaxy, Inc.; 2008.
26. Rawlings AV, Davies A, Cariomusto M, et al. Effect of lactic acid isomers on keratinocyte ceramide synthesis, stratum corneum lipid levels and stratum corneum barrier function. Arch Dermatol Res.1996;288(7):383–390.
27. Lavker RM, Kaidbey K, Leyden JJ. Effects of topical ammonium lactate on cutaneous atrophy from a potent topical corticosteroid. J Am Acad Dermatol. 1992;26:535–544.
28. Dahl MV, Dahl AC. 12% lactate lotion for the treatment of xerosis. Arch Dermatol.1983;119:27–30.
29. Menon GK, Elias PM, Feingold KR. Integrity of the permeability barrier is crucial for maintenance of the epidermal calcium gradient. Br J Dermatol. 1994;130: 139–147.
30. Mao-Qiang M, Feingold KR, Elias PM. Influence of exogenous lipids on permeability barrier recovery in acetone-treated murine skin. Arch Dermatol. 1993;129:728–738.
31. Mao-Qiang M, Brown BE, Wu-Pong S, et al. Exogenous nonphysiologic vs physiologic lipids. Arch Dermatol. 1995;131:809–816.
32. Chamlin SL, Kao J, Frieden IJ, et al. Ceramide-dominant barrier repair lipids alleviate childhood atopic dermatitis: changes in barrier function provide a sensitive indicator of disease activity. J Am Acad Dermatol. 2002;47:198–208.
33. Sugarman JL, Parish LC. Efficacy of a lipid-based barrier repair formulation in moderate-to-severe pediatric atopic dermatitis. J Drugs Dermatol. 2009;8(12):1106–1111.
34. Madaan A. Epiceram for the treatment of atopic dermatitis. Drugs Today (Barc). 2008;44(10):751–755.