
Sarah Grim Hostetler, MD, Division of Dermatology, Ohio State University College of Medicine; Benjamin Kaffenberger, BS, The Ohio State University College of Medicine; Todd Hostetler, MD, Division of Allergy and Immunology, The Ohio State University Medical Center, Columbus, Ohio; Matthew J. Zirwas, MD, Division of Dermatology, Ohio State University College of Medicine
Abstract
Atopic dermatitis is a common, chronic skin condition. A subpopulation of patients may have cutaneous exposure to common airborne proteins exacerbating their disease through direct proteolytic activity, direct activation of proteinase-activated receptor-2 itch receptors, and immunoglobulin E binding. The most common airborne proteins significant in atopic dermatitis include house dust mites, cockroach, pet dander, and multiple pollens. The literature on atopy patch testing, skin-prick testing, and specific IgE is mixed, with greater support for the use of atopy patch test. Patients with airborne proteins contributing to their disease typically have lesions predominately on air-exposed skin surfaces including the face, neck, and arms; a history of exacerbations after exposure to airborne proteins; severe disease resistant to conventional therapies; and concurrent asthma. Treatment strategies include airborne protein avoidance, removal of airborne proteins from the skin, and barrier repair. Further research is needed to establish the benefit of allergen-specific immunotherapy. (J Clin Aesthetic Dermatol. 2010;3(1):22–31.)
Atopic dermatitis (AD) is a common skin condition affecting up to 17 percent of children and two percent of adults in the United States.[1,2] Americans are estimated to spend up to $3.8 billion annually on physician services and prescription drugs for the treatment of AD.[2] A subset of patients have severe AD that is refractory to conventional treatment with topical steroids and moisturizers. Within this group, there may be subpopulations of patients who would benefit from alternative or adjunctive treatment strategies. One group of these patients may have cutaneous exposure to common airborne proteins contributing to AD. This article reviews the evidence for the pathogenesis, laboratory testing, clinical presentation, and treatment options for patients with airborne proteins as a contributing factor to AD.
Pathogenesis of the response to airborne proteins
Patients with AD have a baseline-impaired barrier function that allows proteins to penetrate into the viable epidermis[3] unlike a normally functioning epidermis that prevents protein penetration beyond the stratum corneum. In AD, airborne proteins have the ability to penetrate into the epidermis and worsen AD severity through the following three mechanisms: inherent proteolytic enzyme activity, activation of proteinase-activated receptors-2 (PAR-2), and immunoglobulin E (IgE) binding, leading to increased inflammation (Figure 1).
{kind=link}
First, airborne proteins produced by house dust mites (HDM) and cockroaches have innate proteolytic activity on the skin that can directly contribute to barrier impairment and delayed barrier recovery in patients with AD.4,5 The HDM airborne proteins have been researched extensively and consist primarily of cysteine and serine proteases.[3,4,6] These proteases have been shown to directly disrupt epithelial tight junctions, degranulate eosinophils, and activate keratinocytes, causing increased production of interleukin (IL)-6, IL-8, and granulocyte-macrophage colony-stimulating factor (GM-CSF).[3,4,6-8] These effects contribute to barrier impairment and increased local inflammation. The exogenous proteases also alter the skin’s natural equilibrium between endogenous proteases and endogenous protease inhibitors leading to a delayed barrier recovery in the stratum corneum.[9] The altered barrier function allows airborne proteins, microbes, and other irritants easier access into the epidermis3 where they can interact with local immune cells to initiate the Type-I-immediate and Type-IV-delayed hypersensitivity reactions that are common among patients with AD.[4,5,10] It has also been shown that applying certain weed pollens, animal dander, and molds onto asymptomatic skin can lead to an eczematous reaction in a subgroup of patients with AD.[7] However, the specific proteases associated with weed pollens, animal dander, and molds are not as well described in the basic science literature.
The second mechanism through which airborne proteins exacerbate AD is through direct activation of the PAR-2 receptor on epidermal keratinocytes and dermal unmyelinated nerve fibers. The PAR-2 receptor is crucial to neural transmission of the itch sensation, maintenance of the epidermal calcium ion gradient, and barrier recovery, although the exact mechanisms of action are not well understood.[4,11] The skin biopsies of AD patients typically show an increased density of PAR-2 receptors.11 Both HDM and cockroach proteins have been shown to activate PAR-2 receptors.[6] After binding PAR-2 receptors, cockroach airborne proteins have been shown to cause oscillations in the intracellular calcium levels of keratinocytes that lead to a breakdown in barrier function.[4] The PAR-2 receptor also induces increased nuclear factor kappa-light-chain enhancer of activated B cells (NF-kB) activation and increased production of leukotriene B4 and prostaglandin E2.[4,12] Overall, chronic activation of PAR-2 receptors causes epidermal barrier dysfunction, chronic itch, and delayed barrier recovery.
The final mechanism is classic IgE-mediated allergy. Airborne proteins can bind to specific IgE antibodies and initiate the release of histamine and other inflammatory mediators, resulting in tissue damage.[13,14] In addition, IgE-mediated histamine release from mast cells exacerbates the itch-scratch cycle, which can further worsen AD.[7] The skin of patients with AD has increased numbers of Langerhans cells expressing the high-affinity IgE receptor FceRI compared with the skin of patients without AD.[14] In addition, Novak[15] showed that biopsies taken from the skin of patients with AD during atopy patch test (APT) demonstrated increased chemotactic signals and invasion of dendritic epidermal cells within 24 to 48 hours after protein application.[15] Despite these findings, the incomplete effectiveness of antihistamines in relieving AD-related pruritus suggests there are other mechanisms at work, such as the proteolytic effects and PAR-2 binding noted above.
Laboratory testing for airborne proteins
Because airborne proteins have the potential to contribute to AD, it is important to evaluate possible objective testing for the relevance of certain airborne proteins to an individual patient. These tests include the APT, the skin-prick test (SPT), and specific IgE levels.
First, the APT evaluates Type-IV delayed hypersensitivity responses to a protein. The APT is performed similarly to a standard patch test, except protein allergens are used. A standardized concentration and volume of a protein is applied to the skin under occlusion for 48 hours using either an 8- or 12-mm Finn chamber. An initial reading is sometimes done at 20 minutes to evaluate for immediate urticaria, but the standard readings are done at 48 and 72 hours after application. The APT sites are evaluated for signs of redness and blistering that would indicate a local inflammatory response to the protein. The objective APT result is taken in context of a clinical history of signs or symptoms after exposure to the protein. The procedure essentially assesses the patient’s inflammatory response to a given protein. Classically, the inflammation is thought to be primarily due to Type-IV delayed hypersensitivity reaction. However, there is ongoing investigation to establish if the inflammation may also be due to other processes that increase local inflammation, such as direct proteolytic activity of the protein or binding of PAR-2 receptor.[16]
The APT has the best evidence for identifying AD patients with a relevant airborne protein reaction driving their disease. Several researchers have documented significantly higher rates of positive APT results in patients with an air-exposed pattern of AD when compared to patients with truncal AD lesions.[17,18] Overall, APT results appear highly reproducible.19 The sensitivity ranges between 19 and 75 percent and specificity between 65 and 95 percent.[20–25] Factors influencing this wide range include patient selection by AD severity and distribution, use of skin abrasion in testing methodology, type of protein, and concentration of protein.[20,22–25] While multiple formulations can be used to produce the APT, it has been suggested that the best concentration may be 5,000 to 7,000 protein nitrogen units per gram of concentrate.[18,22] Overall, APT appears to have the highest specificity for assessing airborne protein mediated disease, which makes it the best test, other than clinical history to, predict treatment success. Immunologically, this likely reflects the irritant properties of airborne proteins’ proteolytic enzyme activity and PAR-2 receptor stimulation.
The SPT and specific IgE strictly assess Type-I IgE-mediated allergic responses to a protein, without assessing the ability of the protein to cause inflammation via other mechanisms. The SPT measures the IgE-mediated response to epicutaneous deposition of a protein. It is well known that patients with AD have increased rates of sensitization to a multitude of proteins.[26] Further, as the severity of skin disease increases, the frequency of IgE sensitizations also increases.[26] One study showed that by seven years of age, 80 percent of children with AD were sensitized to at least one airborne protein.[27] It is likely that the increasing sensitization to airborne proteins seen with increasing age is a secondary phenomenon related in part to skin barrier breakdown, mucosal absorption, and increased local inflammation.[28–30] AD patients are more likely to be sensitized to HDM than the majority of other proteins in their environment,[29–35] although it can vary by region.[36] While this test is highly sensitive due to the high prevalence of sensitizations, it is very nonspecific to distinguish airborne, protein-driven AD when compared to patient history. Sensitivities have ranged between 68 and 100 percent while specificities for airborne proteins are between 33 and 71 percent.[20, 22–24] The SPT likely measures a secondary phenomenon to the physiology of AD and is not a reliable marker to identify patients with airborne protein-driven AD.
Lastly, allergic sensitization to an airborne protein can be measured by a specific IgE level. Similar to SPT, researchers have consistently demonstrated a linear association between increasing severity of AD and increasing levels of HDM-specific IgE as well as increasing levels of IgE specific to many other proteins.[37] Again, the altered barrier function of AD likely leads to this secondary phenomenon of increased sensitization to environmental proteins. However, once sensitized, continued exposure to these allergens have the potential to worsen AD by increasing local inflammation. Interestingly, patients with AD were more likely to have elevated HDM-specific IgE levels than patients with asthma; although both had higher levels than the control group.[38] The test is very similar in characteristics to SPT in that it has a high sensitivity, but low specificity. Sensitivities have ranged between 65 and 92 percent and specificities between 33 and 69 percent.[20,22–24] Similar to SPT, specific IgE is not specific enough to identify the subpopulation of patients with airborne protein-driven AD.
Overall, the APT likely provides the most substantial confirmatory evidence that a given airborne protein is relevant for the patient’s disease. The SPT and specific IgE may describe a secondary phenomenon in AD and not the primary driving factor in the disease, and their results should be considered cautiously in a context of a thorough history and physical examination. However, it has clearly been demonstrated that children with positive reactions were significantly less likely to outgrow the disease39 so there may be some prognostic value in the tests.
Clinical signs and symptoms of airborne, protein-driven atopic dermatitis
The best method of identifying patients with airborne, protein-driven AD is likely through a thorough history and physical examination. The most reliable factors include a history of AD exacerbation after exposure to airborne proteins, an air-exposed distribution of eczema, the presence of refractory AD, and concurrent asthma.
First, a history of eczema exacerbations after contact with specific airborne proteins or specific seasonal variation may identify patients likely to have airborne proteins contributing to their disease. The bulk of this evidence is from case series or one-center studies of less than 100 patients.[40–46] For example, Kubota et al[46] described a six-year-old boy with lifelong, severe, generalized AD, mild asthma, and allergic rhinitis.[46] His parents stated he consistently complained of worsening pruritus when he was in closed or air-conditioned rooms. Laboratory evaluation showed a positive APT for HDM, low total serum IgE, and negative HDM-specific IgE. His parents were encouraged to perform HDM avoidance strategies including eliminating all stuffed animals, installing a fine filter in the air conditioner, and thoroughly cleaning the house. One month later, the boy’s AD had completely resolved except for one area on the scrotum. Another case series documented a four-year-old girl who lived on a horse ranch in a humid area of the United States and had recurrent severe dermatitis flares requiring courses of high-dose prednisone, intensive topical steroids, and repeated courses of antibiotics. She had a positive APT to HDM, horse dander, and mold; and a positive SPT to HDM, horse dander, molds, and all pollens. Her lesions cleared completely during a one-month vacation to Phoenix, a city that has been shown to have low concentration of dust mites, and was away from her horse ranch home.[43] Another case series documented an adult with uncontrolled eczema while living in Boston that resolved completely when she moved to Denver (another city with very low levels of HDM) and got rid of her belongings from Boston.[41] Another series described four patients with hand dermatitis flares only after contact with cats and all had positive APT to cat dander.[44] Seasonal flares may also be relevant as one case series describes a patient with severe eczema only during the spring and fall and a positive SPT and APT to oak and ragweed pollen.[41] The subpopulation of airborne protein-driven AD may be more common than previously realized as one study of 253 patients with AD showed 52 percent of patients noticed exacerbations after contact with HDM and 33 percent noticed exacerbations after exposure to grass pollen.[22] Clinical history of exacerbations is an important historical clue to identify this group of AD patients.
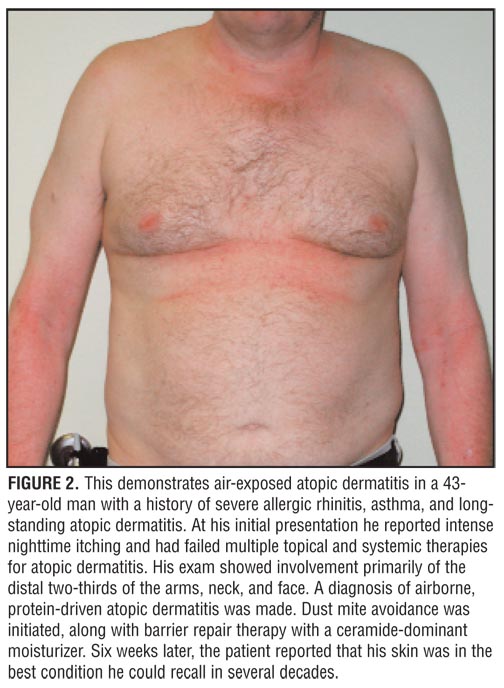
Second, another characteristic of airborne protein-driven AD is the presence of lesions in an air-exposed distribution on the face, neck, décolletage, arms, and lower legs with relative sparing of the trunk (Figure 2).[18,20,44,47] Two studies with 118 and 57 patients, respectively, have shown that patients with an air-exposed eczema pattern were almost twice as likely to have a positive APT to HDM, cat, and/or grass than patients with generalized or flexural AD (69% vs. 39% of patients with a positive APT, p=0.02).[18,20] Further, these patients have also been shown to have a positive APT at lower doses of the protein than patients with generalized or flexural AD47 and frequently show a linear dose-response to airborne protein testing.[20]
{kind=link}
Third, patients with severe AD may be more likely to have airborne proteins contributing to their disease. Their significant baseline barrier dysfunction is likely worsened by airborne proteins’ inherent proteolytic activity and PAR-2 receptor activation. Thus, the barrier becomes even more severely compromised and allows an increased penetration of environmental proteins and chemical irritants as well as increased water loss from the epidermis. Increased exposure to these environmental proteins causes increased frequency of Type-I IgE-mediated and Type-IV delayed contact hypersensitivity reactions that result in increased local inflammation and itch. Specifically, Wahn evaluated more than 2,000 children 13- to 24-months old with AD and found more severe AD disease was associated with an increased frequency of sensitization to airborne proteins (20.5% of patients with mild disease had positive testing compared with 45.4% of patients with severe disease).[26] Three studies including a total of more than 4,000 patients demonstrated increased sensitization to airborne proteins including HDM and cat dander in patients with more severe AD.[17,26,37,48] Overall, it has been established that patients with persistent difficult-to-control AD benefit from a detailed history of exacerbations to identify relevant environmental triggers for their AD.[43]
Although less studied, patients with concurrent allergic asthma may have a higher rate of airborne protein-driven AD. The earliest report of airborne protein-driven AD included two patients with concomitant seasonal worsening of asthma and AD in 1918.[40] A more recent study of 20 patients with AD and asthma found half had a significant exacerbation of their AD after HDM proteins were administered by inhalation only.[49] Interestingly, the patients who had the most severe worsening of their existing eczema lesions also had the most severe baseline AD. Another study used airborne protein inhalation and showed that objective scoring of skin lesions significantly worsened in patients with AD and allergic asthma compared with patients with AD and no asthma (p=0.016).[50]
Treatment strategies for airborne protein-driven atopic dermatitis
The treatment of airborne protein-driven AD may involve a multimodality approach. In addition to standard AD therapy, interventions shown to have possible benefit include airborne protein avoidance, increased frequency of bathing, traditional barrier repair, and systemic immunotherapy. Airborne protein avoidance measures typically include mattress and pillow covers, frequent vacuuming, and frequent laundering of clothing and sheets.
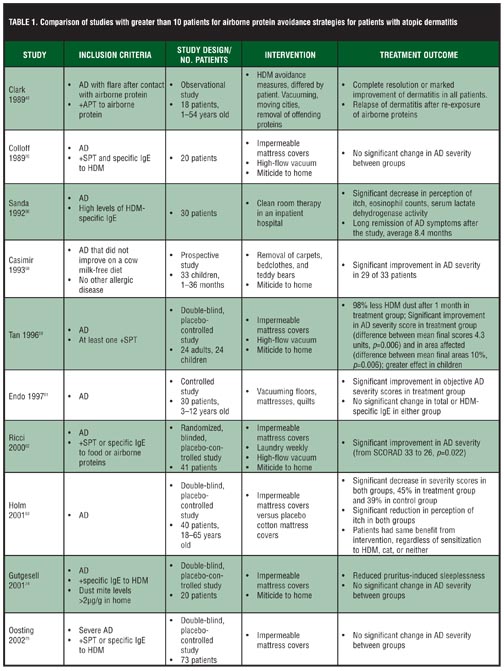
Overall, the data on these novel modalities aimed specifically at airborne-protein reduction are mixed. Therefore, both positive and negative studies are reviewed in the text and in Table 1. This article focuses primarily on HDM because it is the airborne protein with the most evidence for avoidance strategies and because it is likely the most relevant airborne protein for AD. One study showed AD patients were more than three times more likely to have HDM present on their skin when compared to a control group (34.9% of AD patients had HDM detectable on tape stripping of forearms compared with only 7.9% of patients without AD, p<0.001).[51]
{kind=link}
Airborne protein avoidance. Airborne protein avoidance may be an effective strategy to prevent AD or reduce AD severity in high-risk patients. For primary prevention, one study showed infants exposed to more than 1µg of HDM proteins per gram of house dust were four times more likely to have AD than their cohort exposed to less than 1µg of HDM proteins per gram of house dust (21.6% vs. 5.3% of children diagnosed with AD, p=0.0156).[52] There is a linear increase in the incidence of AD correlating with increased exposure to HDM, with research showing 4.9 percent of individuals with low HDM levels in the home had AD, compared with 13.9 percent of individuals with very high HDM levels in the home had AD.[53] Follow-up studies have demonstrated that children at high-risk for AD who were randomized to airborne-protein avoidance and control groups showed a significant reduction in AD in the therapeutic group at one year, which remained consistent until the eighth and final year of the study.[54–57]
For secondary prevention after diagnosis of AD, multiple studies have shown improvement in AD severity after initiating HDM avoidance strategies.[41–43,46,58] This is particularly true in patients with positive APTs and SPTs to HDM.[41–43] Several randomized, controlled trials showed significant improvement in patients treated in the therapeutic group despite significant decrease in mite levels in both active and placebo groups.[59–63]
It is important to note that a substantial number of studies have found no difference in AD frequency or severity with airborne protein avoidance measures.[64–73] One study of 642 infants from the general population demonstrated no association between exposure to HDM or cats and subsequent development of AD.[64,65] In another study, AD was actually more likely in the HDM-avoidance group after one year, but there was no significant difference between the groups at the three-year follow up.[68–70] Several of these trials have documented decreased levels of HDM with no change in the severity of AD.[74–76]
Factors influencing the differing results are likely related to patient selection, relevance of HDM proteins, effects of placebo interventions, and baseline HDM levels. Studies varied greatly in their patient selection. Specifically, studies with positive results from HDM avoidance measures were more likely to select patients with more severe AD, a clinical history of exacerbation after airborne protein exposure, and/or an air-exposed distribution of lesions. Further, some studies did not use objective testing of APT, SPT, or specific IgE to assess the likely relevance of airborne proteins. If APT testing was used, there was variation in test protocol as some used tape stripping, scratching, or other methods of abrasion in addition to the standard patch-test methodology. Third, several of the negative studies found HDM concentrations decreased both with the intervention and with the placebo.[66–70,77,78] For example, impermeable mattress covers for the treatment groups and cotton mattress covers for the intervention group both caused a significant reduction in HDM levels in one study.[63] It is possible the intervention was effective from baseline, but was not detected due to partial effect of the placebo. Lastly, baseline levels of airborne proteins, HDM in particular, can vary greatly based on geographic variation.[79] High mite levels are most closely linked to areas with high humidity.[79] Studies conducted in communities with low levels of airborne proteins may not have shown benefit because the net change in protein levels was not significant, compared with studies conducted in areas with high baseline levels of the proteins. While the literature agrees that reducing HDM within the house is possible, the preponderance of evidence has not shown efficacy in AD prevention. It is possible that merely decreasing HDM levels at home still allows for too many confounding variables and further control needs to be exercised in future randomized, placebo-controlled trials. Future studies should identify subjects via strict clinical criteria that select patients with AD that is likely to be airborne-protein driven, use specific APT methodology, and include direct measurement of HDM levels before and after intervention to better assess for potential responders.
The evidence for decreased incidence and severity of AD through reduction of HDM levels will be reviewed by modality. It is important to examine the evidence for each modality before recommending it to patients as each generates both time and monetary costs to patients and their families.
Mattress and pillow covers. Several studies have shown a decreased incidence or decreased severity of AD in patients using allergen-impermeable mattress and pillow covers regularly.[52,59,60,63,74,75] One study followed 931 infants through the first three years of life in an area with high HDM levels and found a four-fold higher incidence of AD among the neonates from homes with high HDM levels that were not using the mattress covers (21.6% of neonates with AD in the control group vs. 5.3% of neonates with AD from homes using mattress covers, p=0.016).[52] Other research selected patients with severe AD[75] or high HDM levels[74] and showed a significant reduction in both the severity of patients’ skin lesions and in their objective itching scores with regular use of impermeable mattress and pillow covers. Holm et al[63] used an impermeable mattress cover as the intervention and a cotton mattress cover as the placebo. They found both groups had decreased levels of HDM, a significant reduction in AD severity scores, and a significant reduction in itch.[63] Interestingly, this study and the majority of these studies found no correlation with SPT results or HDM-specific IgE levels and response to therapy, illustrating the likely primary effects of proteolytic and PAR-2 activity for this protein.[52,63] It is important to note most of these studies combined the mattress cover with other interventions, such as miticides (Table 1).
Frequent vacuuming. Frequent vacuuming in the house has been shown to decrease the likelihood of AD in the first year of life.[52,80] Several studies have shown significant improvement in clinical AD scores after weekly vacuuming of floors, mattresses, and quilts.[59–61] Interestingly, their HDM-specific IgE levels were unchanged in most studies that measured them. Removal of carpet in the home resulted in significant improvement in 29 of 33 toddlers with AD.[58]
Frequent laundry. One study showed infants of mothers with a high HDM-protein load on their pajamas were more than three times more likely to be diagnosed with AD than infants of mothers with low HDM-protein loads on their pajamas (OR 3.45, 95% CI 1.63–7.01).80 Little research has been done on this intervention to date, but it may be an appropriate recommendation to patients as it is relatively inexpensive and has easy access.
Frequent bathing. Bathing with or without soap can remove airborne proteins from the skin and may have a place in the treatment of AD. Use of emollients afterwards is important. Frequent neonatal bathing has been shown to decrease the likelihood of AD in the first year of life.[52,80] Two observational trials with 900 patients total showed benefit of bathing once or more per day.[80,81] A randomized, controlled trial measured the clinical response in school children with AD who showered during the school day in addition to their regular bathing routine and found a significant improvement after four weeks with those with the greatest AD severity having the greatest benefit.[82] More research needs to be performed to determine if increased showers are indeed beneficial. However, given the inexpensive nature and easy access to home showering, showering twice a day may be worth a trial in patients likely to have airborne proteins contributing to their disease.
Barrier repair. Barrier repair is a foundational therapeutic goal for all patients with AD. Barrier repair is likely of particular importance for patients with airborne protein-driven AD as the expected outcome of barrier repair would be reduced penetration of these proteins. In particular, ceramides are an integral component to the stratum corneum and may be more important than physiological ratios of lipids in AD.[83,84] A ceramide-dominant ointment, TriCeram (Osmotics Comeceuticals, Denver, Colorado), proved efficacious in barrier repair for 22 of 24 patients after three weeks of therapy.[85,86] Barrier repair is an important mainstay of therapy for all patients with AD and particularly for those with relevant exposures to airborne proteins.
Allergen-specific immunotherapy. Allergen-specific immunotherapy is defined as “the repeated administration of specific allergens to patients with IgE-mediated conditions for the purpose of providing protection against the allergic symptoms and inflammatory reactions associated with natural exposure to these allergens.”[87] While multiple methods of immunotherapy exist, subcutaneous and sublingual immunotherapies are thought to be the most efficacious and best tolerated.88 Subcutaneous immunotherapy is the most widely used form in the United States, and sublingual immunotherapy is used mostly in Europe, but it is gaining interest in the United States. However, there are still no FDA-approved sublingual immunotherapy products.[89]
Current recommendations state that while there are some encouraging studies, the collective data are too limited and weak to consider allergen-specific immunotherapy effective for patients with AD and sensitization to airborne proteins.[5,87,90–92] Several studies have reviewed the literature on allergen-specific immunotherapy for patients with AD.[5,92] The main weaknesses of previous studies are that they are observational instead of prospective, not blinded, not placebo-controlled, of insufficient power, and have high drop-out rates. Further, it is difficult to compare these studies due to lack of consensus-based international guidelines on scoring AD severity; different allergens, extracts, application schedules, and inclusion criteria used between studies; and a lack of standardized topical treatment to go along with specific immunotherapy.
As mentioned previously, there have been some promising studies. Werfel et al[93] performed a multicenter, randomized, blinded, dose-response study with HDM subcutaneous immunotherapies in patients with AD and HDM sensitivity and demonstrated that objective scoring of AD declined significantly in a dose-dependent manner. The use of topical steroids was also significantly reduced in patients receiving higher doses.[93] Bussmann5 et al reported a 70.8-percent mean proportion of improvement of AD using specific immunotherapy by performing a combined statistical analysis of seven comparable observational studies. In addition, Pajno et al[94] studied sublingual immunotherapies in HDM-sensitized children in a randomized, placebo-controlled manner and found a difference between the treatment group versus placebo in objective scoring of AD and medication use at nine months, but only in patients with mild-to-moderate AD.[94] However, they also reported that two of the patients discontinued sublingual immunotherapies due to exacerbation of their AD, which has also been previously reported in other studies.[5] In contrast, there have also been studies showing no benefit over placebo.[95]
In summary, much of the published data suggest a therapeutic benefit of allergen-specific immunotherapy in AD, but generalized conclusions and recommendations cannot be made until more randomized, double-blind, placebo-controlled trials are completed.
Summary
A subpopulation of AD patients may have a reaction to common airborne proteins exacerbating their disease. The reactions to airborne proteins are likely mediated by multiple mechanisms, including direct proteolytic activity leading to degradation of the stratum corneum, direct activation of PAR-2 itch receptors, and IgE binding causing increased local inflammation. The most common airborne proteins that have been shown to be significant in AD include HDM, cockroach, pet dander, and multiple pollens. The literature on APT, skin-prick testing, and specific IgE is mixed, with greater support for the use of APT results to identify this subpopulation. Patients likely to have airborne proteins contributing to their disease typically have lesions predominately on air-exposed skin surfaces including the face, neck, and arms; a history of exacerbations after exposure to airborne proteins; severe AD resistant to conventional therapies; and concurrent asthma. Possible treatment strategies include airborne protein avoidance, frequent bathing, and barrier repair. Further research is needed to establish the benefit of allergen-specific immunotherapy.
References
1. Ellis CN, Drake LA, Prendergast MM, et al. Cost of atopic dermatitis and eczema in the United States. J Am Acad Dermatol. 2002;46:361–370.
2. Mancini AJ, Kaulback K, Camlin SL. The socioeconomic impact of atopic dermatitis in the United States: a systematic review. Pediatr Dermatol. 2008;25(1):1–6.
3. Nakamura T, Hirasawa Y, Takai T, et al. Reduction of skin barrier function by proteolytic activity of a recombinant house dust mite major allergen der f 1. J Invest Dermatol. 2006;126(12):2719–2723.
4. Jeong SK, Kim HJ, Youm JK, et al. Mite and cockroach allergens activate protease-activated receptor 2 and delay epidermal permeability barrier recovery. J Invest Dermatol. 2008;128(8):1930–1939.
5. Bussmann C, Böckenhoff A, Henke H, Werfel T, Novak N. Does allergen-specific immunotherapy represent a therapeutic option for patients with atopic dermatitis? J Allergy Clin Immunol. 2006;118(6):1292–1298.
6. Kato T, Takai T, Fujimura T, et al. Mite serine protease activates protease-activated receptor-2 and induces cytokine release in human keratinocytes. Allergy. 2009;64(9):1366–1374. Epub 2009 Mar 23.
7. Werfel T. The role of leukocytes, keratinocytes, and allergen-specific IgE in the development of atopic dermatitis. J Invest Dermatol. 2009;129(8):1878–1891.
8. Wan H, Winton HL, Soeller C, et al. The transmembrane protein occludin of epithelial tight junctions is a functional target for serine peptidases from faecal pellets of dermatophagoides pteronyssinus. Clin Exp Allergy. 2001;31(2):279–294.
9. Meyer-Hoffert U. Reddish, scaly, and itchy: how proteases and their inhibitors contribute to inflammatory skin diseases. Arch Immunol Ther Exp (Warsz). 2009;57(5):345–354.
10. Boralevi F, Hubiche T, Leaute-Labreze C, et al. Epicutaneous aeroallergen sensitization in atopic dermatitis infants—determining the role of epidermal barrier impairment. Allergy. 2008;63(2):205–210.
11. Steinhoff M, Neisius U, Ikoma A, et al. Proteinase-activated receptor-2 mediates itch: a novel pathway for pruritus in human skin. J Neurosci. 2003;23(15):6176–6180.
12. Zhu Y, Wang XR, Peng C, et al. Induction of leukotriene B4 and prostaglandin E2 release from keratinocytes by protease-activated receptor-2-activating peptide in ICR mice. Int Immunopharmacol. In Press, Corrected Proof.
13. Shakib F, Schulz O, Sewell H. A mite subversive: Cleavage of CD23 and CD25 by der p 1 enhances allergenicity. Immunol Today. 1998;19(7):313–316.
14. Beltrani VS. The role of house dust mites and other aeroallergens in atopic dermatitis. Clin Dermatol. 2003;21: 177–182.
15. Novak N. New insights into the mechanism and management of allergic diseases: atopic dermatitis. Allergy. 2009;64:265–275.
16. Deleuran M, Ellingsen AR, Paludan K, Schou C, Thestrup-Pedersen K. Purified der p1 and p2 patch tests in patients with atopic dermatitis: evidence for both allergenicity and proteolytic irritancy. Acta Derm Venereol. 1998;78(4): 241–243.
17. Holm L, van Hage-Hamsten M, Ohman S, Scheynius A. Sensitization to allergens of house-dust mite in adults with atopic dermatitis in a cold temperature region. Allergy. 1999;54(7):708–715.
18. Darsow U, Vieluf D, Ring J. The atopy patch test: an increased rate of reactivity in patients who have an air-exposed pattern of atopic eczema. Br J Dermatol. 1996;135(2):182–186.
19. Giusti F, Seidenari S. Reproducibility of atopy patch tests with dermatophagoides: A study on 85 patients with atopic dermatitis. Contact Dermatitis. 2004;50(1):18–21.
20. Ring J, Darsow U, Gfesser M, Vieluf D. The ‘atopy patch test’ in evaluating the role of aeroallergens in atopic eczema. Int Arch Allergy Immunol. 1997;113(1-3):379–383.
21. Wistokat-Wülfing A, Schmidt P, Darsow U, et al. Atopy patch test reactions are associated with T lymphocyte-mediated allergen-specific immune responses in atopic dermatitis. Clin Exp Allergy. 1999;29(4):513–521.
22. Darsow U, Vieluf D, Ring J. Evaluating the relevance of aeroallergen sensitization in atopic eczema with the atopy patch test: a randomized, double-blind multicenter study. atopy patch test study group. J Am Acad Dermatol. 1999;40(2):187–193.
23. Darsow U, Laifaoui J, Kerschenlohr K, et al. The prevalence of positive reactions in the atopy patch test with aeroallergens and food allergens in subjects with atopic eczema: a European multicenter study. Allergy. 2004;59(12):1318–1325.
24. Darsow U, Behrendt H, Ring J. Gramineae pollen as trigger factors of atopic eczema: Evaluation of diagnostic measures using the atopy patch test. Br J Dermatol. 1997;137(2):201–207.
25. Samochocki Z, Owczarek W, Zabielski S. Can atopy patch tests with aeroallergens be an additional diagnostic criterion for atopic dermatitis? Eur J Dermatol. 2006;16(2):151–154.
26. Wahn U, Warner J, Simons FE, et al. EPAAC Study Group. IgE antibody responses in young children with atopic dermatitis. Pediatr Allergy Immunol. 2008;19(4):332–336.
27. Gustafsson D, Sjoberg O, Foucard T. Sensitization to food and airborne allergens in children with atopic dermatitis followed up to 7 years of age. Pediatr Allergy Immunol. 2003;14(6):448–452.
28. Hon KL, Leung TF, Ching G, et al. Patterns of food and aeroallergen sensitization in childhood eczema. Acta Paediatr. 2008;97(12):1734–1737.
29. Arshad SH, Tariq SM, Matthews S, Hakim E. Sensitization to common allergens and its association with allergic disorders at age 4 years: a whole population birth cohort study. Pediatrics. 2001;108(2):E33.
30. Wang IJ, Lin YT, Yang YH, et al. Correlation between age and allergens in pediatric atopic dermatitis. Ann Allergy Asthma Immunol. 2004;93(4):334–338.
31. Stajminger G, Marinovic-Kulisic S, Lipozencic J, Pastar Z. Most common inhalant allergens in atopic dermatitis, atopic dermatitis/allergic rhinitis, and atopic dermatitis/bronchial asthma patients: a five-year retrospective study. Acta Dermatovenerol Croat. 2007;15(3):130–134.
32. Goon A, Leow YH, Chan YH, Ng SK, Goh CL. Atopy patch testing with aeroallergens in patients with atopic dermatitis and controls in singapore. Clin Exp Dermatol. 2005;30(6):627–631.
33. de Benedictis FM, Franceschini F, Hill D, et al. EPAAC Study Group. The allergic sensitization in infants with atopic eczema from different countries. Allergy. 2009;64(2):295–303.
34. Samochocki Z, Owczarek W, Rujna P, Raczka A. Hypersensitivity to aeroallergens in adult patients with atopic dermatitis develops due to the different immunological mechanisms. Eur J Dermatol. 2007;17(6):520–524.
35. Montealegre F, Meyer B, Chardon D, et al. Comparative prevalence of sensitization to common animal, plant and mould allergens in subjects with asthma, or atopic dermatitis and/or allergic rhinitis living in a tropical environment. Clin Exp Allergy. 2004;34(1):51–58.
36. Clausen M, Kristjansson S, Haraldsson A, Bjorksten B. High prevalence of allergic diseases and sensitization in a low allergen country. Acta Paediatr. 2008;97(9):1216–1220.
37. Schäfer T, Heinrich J, Wjst M, et al. Association between severity of atopic eczema and degree of sensitization to aeroallergens in schoolchildren. J Allergy Clin Immunol. 1999;104(6):1280–1284.
38. Scalabrin DM, Bavbek S, Perzanowski MS, et al. Use of specific IgE in assessing the relevance of fungal and dust mite allergens to atopic dermatitis: A comparison with asthmatic and nonasthmatic control subjects. J Allergy Clin Immunol. 1999;104(6):1273–1279.
39. Pajno GB, Peroni DG, Barberio G, Pietrobelli A, Boner AL. Predictive features for persistence of atopic dermatitis in children. Pediatr Allergy Immunol. 2003;14(4):292–295.
40. Walker JC. Causation of eczema, urticaria, and angioneurotic edema by proteins other than those derived from foods. JAMA. 1918;70:897–900.
41. Adinoff AD, Tellez P, Clark RA. Atopic dermatitis and aeroallergen contact sensitivity. J Allergy Clin Immunol. 1988;81(4):736–742.
42. Clark RA, Adinoff AD. Aeroallergen contact can exacerbate atopic dermatitis: patch tests as a diagnostic tool. J Am Acad Dermatol. 1989;21(4):863–869.
43. Clark RA, Adinoff AD. The relationship between positive aeroallergen patch test reactions and aeroallergen exacerbations of atopic dermatitis. Clin Immunol Immunopathol. 1989;53(2):S132–S140.
44. Ponyai G, Hidvegi B, Nemeth I, et al. Contact and aeroallergens in adulthood atopic dermatitis. J Eur Acad Dermatol Venereol. 2008;22(11):1346–1355.
45. Kerschenlohr K, Darsow U, Burgdorf WH, Ring J, Wollenberg A. Lessons from atopy patch testing in atopic dermatitis. Curr Allergy Asthma Rep. 2004;4(4):285–289.
46. Kubota Y, Imayama S, Hori Y. Reduction of environmental mites improved atopic dermatitis patients with positive mite-patch tests. J Dermatol. 1992;19(3):177–180.
47. Darsow U, Ring J. Airborne and dietary allergens in atopic eczema: A comprehensive review of diagnostic tests. Clin Exp Dermatol. 2000;25(7):544–551.
48. Hon KL, Leung TF, Lam MC, et al. Which aeroallergens are associated with eczema severity? Clin Exp Dermatol. 2007;32(4):401–404.
49. Tupker RA, De Monchy JG, Coenraads PJ, Homan A, van der Meer JB. Induction of atopic dermatitis by inhalation of house dust mite. J Allergy Clin Immunol. 1996;97(5):1064–1070.
50. Brinkman L, Aslander MM, Raaijmakers JA, et al. Bronchial and cutaneous responses in atopic dermatitis patients after allergen inhalation challenge. Clin Exp Allergy. 1997;27(9):1043–1051.
51. Teplitsky V, Mumcuoglu KY, Babai I, et al. House dust mites on skin, clothes, and bedding of atopic dermatitis patients. Int J Dermatol. 2008;47(8):790–795.
52. Huang JL, Chen CC, Kuo ML, Hsieh KH. Exposure to a high concentration of mite allergen in early infancy is a risk factor for developing atopic dermatitis: a 3-year follow-up study. Pediatr Allergy Immunol. 2001;12(1):11–16.
53. Schafer T. The impact of allergy on atopic eczema from data from epidemiological studies. Curr Opin Allergy Clin Immunol. 2008;8(5):418–422.
54. Arshad SH, Matthews S, Gant C, Hide DW. Effect of allergen avoidance on development of allergic disorders in infancy. Lancet. 1992;339(8808):1493–1497.
55. Hide DW, Matthews S, Matthews L, et al. Effect of allergen avoidance in infancy on allergic manifestations at age two years. J Allergy Clin Immunol. 1994;93(5):842–846.
56. Hide DW, Matthews S, Tariq S, Arshad SH. Allergen avoidance in infancy and allergy at 4 years of age. Allergy. 1996;51(2):89–93.
57. Arshad SH, Bateman B, Sadeghnejad A, Gant C, Matthews SM. Prevention of allergic disease during childhood by allergen avoidance: the Isle of Wight prevention study. J Allergy Clin Immunol. 2007 /2;119(2):307–313.
58. Casimir GJ, Duchateau J, Gossart B, et al. Atopic dermatitis: role of food and house dust mite allergens. Pediatrics. 1993;92(2):252–256.
59. Tan BB, Weald D, Strickland I, Friedmann PS. Double-blind controlled trial of effect of housedust-mite allergen avoidance on atopic dermatitis. Lancet. 1996;347(8993):15–18.
60. Friedmann PS, Tan BB. Mite elimination—clinical effect on eczema. Allergy. 1998;53(48):97–100.
61. Endo K, Fukuzumi T, Adachi J, et al. Effect of vacuum cleaning of room floors and bed clothes of patients on house dust mites counts and clinical scores of atopic dermatitis. A double blind control trial. Aerugi. 1997;46(10):1013–1024.
62. Ricci G, Patrizi A, Specchia F, et al. Effect of house dust mite avoidance measures in children with atopic dermatitis. Br J Dermatol. 2000;143(2):379–384.
63. Holm L, Öhman S, Bengtsson Å, Hage-Hamsten Mv, Scheynius A. Effectiveness of occlusive bedding in the treatment of atopic dermatitis—a placebo-controlled trial of 12 months’ duration. Allergy. 2001;56(2):152–158.
64. Harris JM, Cullinan P, Williams HC, et al. Environmental associations with eczema in early life. Br J Dermatol. 2001;144(4):795–802.
65. Harris JM, Williams HC, White C, et al. Early allergen exposure and atopic eczema. Br J Dermatol. 2007;156(4):698–704.
66. Custovic A, Simpson BM, Simpson A, et al. Manchester asthma and allergy study: Low allergen environment can be achieved and maintained during pregnancy and in early life. J Allergy Clin IMmunol. 2000;105:252–258.
67. Woodcock A, Lowe LA, Murray CS, et al. Early life environmental control: Effect on symptoms, sensitization, and lung function at age 3 years. Am J Respir Crit Care Med. 2004;170(4):433–439.
68. van Strien RT, Koopman LP, Kerkhof M, et al. Mattress encasings and mite allergen levels in the prevention and incidence of asthma and mite allergy study. Clin Exp Allergy. 2003;33(4):490–495.
69. Koopman LP, van Strien RT, Kerkhof M, et al. Placebo-controlled trial of house dust mite-impermeable mattress covers: Effect on symptoms in early childhood. Am J Respir Crit Care Med. 2002;166(3):307–313.
70. Corver K, Kerkhof M, Brussee JE, et al. House dust mite allergen reduction and allergy at 4 yr: Follow up of the PIAMA-study. Pediatr Allergy Immunol. 2006;17(5): 329–336.
71. Horak F, Matthews S, Ihorst G, et al. Effect of mite-impermeable mattress encasings and an educational package on the development of allergies in a multinational randomized, controlled birth-cohort study—24 months results of the study of prevention of allergy in children in europe. Clin Exp Allergy. 2004;34(8):1220–1225.
72. Mihrshahi S, Peat JK, Marks GB, et al. Eighteen-month outcomes of house dust mite avoidance and dietary fatty acid modification in the childhood asthma prevention study (CAPS). J Allergy Clin Immunol. 2003;111(1):162–168.
73. Tsitoura S, Nestoridou K, Botis P, et al. Randomized trial to prevent sensitization to mite allergens in toddlers and preschoolers by allergen reduction and education: one-year results. Arch Pediatr Adolesc Med. 2002;156(10): 1021–1027.
74. Gutgesell C, Heise S, Seubert S, et al. Double-blind placebo-controlled house dust mite control measures in adult patients with atopic dermatitis. Br J Dermatol. 2001;145(1):70–74.
75. Oosting AJ, de Bruin-Weller MS, Terreehorst I, et al. Effect of mattress encasings on atopic dermatitis outcome measures in a double-blind, placebo-controlled study: the dutch mite avoidance study. J Allergy Clin Immunol. 2002;110(3):500–506.
76. Colloff MJ, Lever RS, McSharry C. A controlled trial of house dust mite eradication using natamycin in homes of patients with atopic dermatitis: effect on clinical status and mite populations. Br J Dermatol. 1989;121(2):199.
77. Custovic A, Simpson BM, Simpson A, Kissen P, Woodcock A. Effect of environmental manipulation in pregnancy and early life on respiratory symptoms and atopy during first year of life: A randomised trial. Lancet. 2001 /7/21/;358(9277):188–193.
78. Capristo C, Romei I, Boner AL. Environmental prevention in atopic eczema dermatitis syndrome (AEDS) and asthma: avoidance of indoor allergens. Allergy. 2004;59 Suppl 78:53–60.
79. Arlian L, Morgan M, Neal JS. Dust mite allergens: ecology and distribution. Curr Allergy Asthma Rep. 2002;2(5):401.
80. Miyake Y, Ohya Y, Tanaka K, et al. Home environment and suspected atopic eczema in japanese infants: The Osaka Maternal and Child Health Study. Pediatr Allergy Immunol. 2007;18(5):425–432.
81. Mochizuki H, Muramatsu R, Tadaki H, et al. Effects of skin care with shower therapy on children with atopic dermatitis in elementary schools. Pediatr Dermatol. 2009;26(2):223–225.
82. Kameyoshi Y, Tanaka T, Mochizuki M, et al. Taking showers at school is beneficial for children with severer atopic dermatitis. Arerugi. 2008;57(2):130–137.
83. Vavrova K, Zbytovska J, Palat K, et al. Ceramide analogue 14S24 ((S)-2-tetracosanoylamino-3-hydroxypropionic acid tetradecyl ester) is effective in skin barrier repair in vitro. Eur J Pharm Sci. 2004;21:581–587.
84. Vavrova K, Hrabalek A, Mac-Mary S, Humbert P, Muret P. Ceramide analogue 14S24 selectively recovers perturbed human skin barrier. Br J Dermatol. 2007;157:704–712.
85. Chamlin S, Frieden I, Fowler A, et al. Ceramide-dominant, barrier-repair lipids improve childhood atopic dermatitis. Arch Dermatol. 2001;137:1110–1112.
86. Chamlin S, Kao J, Frieden I, et al. Ceramide-dominant barrier repair lipids alleviate childhood atopic dermatitis: changes in barrier function provide a sensitive indicator of disease activity. J Am Acad Dermatol. 2002;47:198–208.
87. Cox L, Li JT, Nelson H, Lockey R. Allergen immunotherapy: a practice parameter second update. J Allergy Clin Immunol. 2007;120(3):S25–S85.
88. Nelson HS. Allergen immunotherapy: Where is it now? J Allergy Clin Immunol. 2007;119(4):769–777.
89. Cox LS, Linnemann D, Nolte H, et al. Sublingual immunotherapy: a comprehensive review. J Allergy Clin Immunol. 2006;117(5):1021–1035.
90. Hsu C, Wang L. Emerging treatment of atopic dermatitis. Clin Rev Allergy Immunol. 2007 12/01;33(3):199–203.
91. Boguniewicz M, Schmid-Grendelmeier P, Leung DYM. Atopic dermatitis. J Allergy Clin Immunol. 2006;118(1):40–43.
92. Mastrandrea F. The potential role of allergen-specific sublingual immunotherapy in atopic dermatitis. Am J Clin Dermatol. 2004;5(5):281–294.
93. Werfel T, Breuer K, Ruéff F, et al. Usefulness of specific immunotherapy in patients with atopic dermatitis and allergic sensitization to house dust mites: a multi-centre, randomized, dose-response study. Allergy. 2006;61(2): 202–205.
94. Pajno GB, Caminiti L, Vita D, et al. Sublingual immunotherapy in mite-sensitized children with atopic dermatitis: a randomized, double-blind, placebo-controlled study. J Allergy Clin Immunol. 2007;120(1):164–170.
95. Glover M, Atherton DJ. A double-blind controlled trial of hyposensitization to dermatophagoides pteronyssinus in children with atopic eczema. Clin Exp Allergy. 1992;22(4):440.
96. Sanda T, Yasue T, Oohashi M, Yasue A. Effectiveness of house dust-mite allergen avoidance through clean room therapy in patients with atopic dermatitis. J Allergy Clin Immunol. 1992;89(3):653–657