
Susan Van Dyke, MD, Van Dyke Laser & Skin, Paradise Valley, Arizona; Geoffrey P. Hays (MS1), Creighton University Medical Center, Omaha, Nebraska; Anthony E. Caglia, MD, Derm Aesthetics & Laser Center, Dallas, Texas; Michael Caglia, MD, Texas Tech University Health Sciences Center, Lubbock, Texas
Abstract
Injectable fillers are normally well tolerated by patients with little or no adverse effects. The most common side effects include swelling, redness, bruising, and pain at the injection site. This report describes three cases in which patients injected with a hyaluronic acid-derived injectable filler that is premixed with lidocaine developed adverse reactions including persistent swelling, pain, and nodule formation. Two of the three patients’ abscesses were cultured for aerobic and anaerobic bacteria and mycobacterium. All three cultures were negative. Abscess persistence in all cases necessitated physical removal and/or enzymatic degradation with hyaluronidase. The effects subsided only after the product had been removed. Two of these patients were subsequently treated with other hyaluronic acid-derived dermal fillers without adverse events. (J Clin Aesthetic Dermatol. 2010;3(5):32–35.)
Injectable fillers are commonly used for soft tissue augmentation in areas of collagen loss. Adverse events with these materials are rare.[1] Hyaluronic acid (HA)-based injectables as well as polylactic acid (PLA)-based fillers, when injected into the glabella, are reported to have a lower incidence of complications compared to permanent fillers.[2] The most serious reactions can be reduced through a greater understanding of the anatomy of the area being treated as well as proper technique employed to avoid blood vessels.[3] The reports of adverse reactions in the use of PLA-based injectables has declined in recent years due to an increase in physician education and standardized practice.[4] Although rare, hypersensitivity and inflammatory reactions likely due to contamination of byproducts with bacterial fermentation are the most common adverse reactions associated with HA-based fillers.[5] As new products enter the market, however, adverse reactions may become more common.
Elevess (Anika Therapeutics, Inc., Bedford, Massachusetts), an HA-based injectable filler, was approved by the United States Food and Drug Administration (FDA) in 2006 for cosmetic use. It is a cross-linked hyaluronan gel suspended in a buffer solution with 0.3% lidocaine hydrochloride. It is indicated for injection for the correction of moderate-to-severe facial wrinkles.[6]
In the authors’ experience, anecdotal evidence is surfacing that details adverse events with injectable Elevess including edema, pain, nodules, redness, purpura, and formation of granulomas and purulent exudate. This report describes three such cases.
CASE REPORT 1
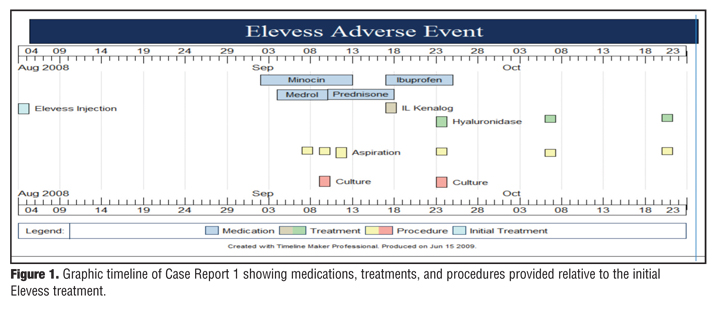
A 51-year-old woman with a past history of using dermatological fillers without adverse events presented for additional filler for the nasolabial and marionette areas. Her last treatment was three months prior and consisted of two syringes of Perlane (Medicis Pharmaceutical Corporation, Scottsdale, Arizona) in the nasolabial and marionette areas. Partial correction was present. She had no relevant medical history other than penicillin allergy. On August 4, 2008, she was treated with two syringes of Elevess in the nasolabial folds and marionette regions. Over the course of the next three months, the patient was seen 12 times because of severe swelling and pain at the nasolabial and marionette areas (Figure 1)
{kind=link}
The patient immediately experienced minor swelling appropriate to the procedure, but presented 30 days after the injections with continued swelling, increased firmness over the treatment sites, and a 6mm nodule above the left lip. Because infection was initially suspected as the cause of the inflammation, minocycline was prescribed (50mg twice daily for 10 days). A methylprednisolone dose pack was also prescribed two days later when the patient complained of increasing swelling (Figure 2). After three days of methylprednisolone, the areas had improved and become notably fluctuant. Two fluctuant nodules were aspirated, yielding over 1cc of yellow, opaque, slightly hemorrhagic fluid from each site. The patient experienced immediate pain relief and flattening of the areas. A second aspiration was performed after the areas refilled within 48 hours. Aspirations were performed four more times on Days 39, 51, 64, and 78 post-Elevess injection to relieve pressure and pain. Each aspiration yielded yellowish, cloudy, odorless, thick, slightly hemorrhagic fluid. The aspirant from Days 37 and 51 post-Elevess were cultured for aerobic and anaerobic bacteria and mycobacterium and was found to be sterile.
{kind=link}
On Day 38, the patient was put on prednisone (20mg twice daily for 7 days), which was rapidly tapered due to intolerance of the medication. Intralesional triamcinolone (0.5cc of 5mg/cc) was injected on Day 45. The patient was started on ibuprofen 600mg every eight hours. She reported that her swelling and tenderness had diminished except for the right upper nasolabial area. Hyaluronidase (100units/cc) was injected into the treatment sites on Days 51, 64, and 78 following aspirations in an effort to break down any filler that might be stimulating the patient’s chronically recurring fluctuant nodules. With each aspiration/hyaluronidase injection, the patient experienced immediate relief and improvement. Signs and symptoms subsided 101 days post-Elevess injection.
Despite the adverse reaction to Elevess, the patient requested to be treated with Juvederm (Allergan, Inc., Irvine, California) several weeks following resolution of her symptoms. She understood the risk of reactivating the reaction. Juvederm Ultra was injected into her upper nasolabial folds bilaterally without incident. Eleven months after receiving Elevess, the patient is symptom free.
CASE REPORT 2
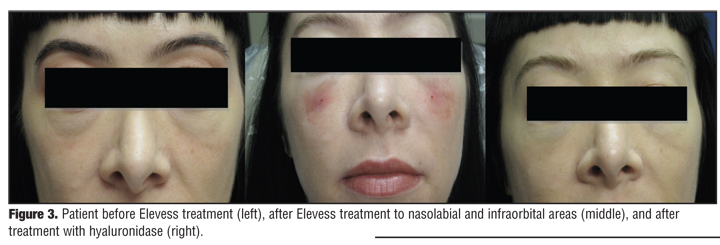
A 41-year-old Caucasian female with a past history of using Juvederm Ultra Plus on multiple occasions in the nasolabial folds, lips, and infraorbital area (tear trough) without prior adverse events, presented for treatment of her tear trough area. Her last treatment was 10 months prior and consisted of one syringe of Juvederm Ultra Plus to the nasolabial folds and tear trough regions. Her only relevant medical history was allergy to amoxicillin and seasonal allergies. On February 26, 2009, the patient was treated with two syringes of Elevess in the nasolabial and infraorbital (tear trough) area. Over the course of the next four months, the patient was seen eight times for complaints of swelling, pain, and skin color changes in the areas treated. The patient initially developed swelling to these areas that subsided after several days. Subsequently, on Day 10, she developed tenderness, skin color changes that resembled purpura, swelling, and a palpable nodule under her right eye in the injection area. Skin temperatures recorded with the Raytek IF device were 34.9ºC on the affected side and 32.9ºC on the unaffected side. The clinician believed the patient had cellulitis and placed her on azithromycin 250mg for five days. On Day 14, she developed increased erythema, swelling, and tenderness with a nodule measuring 1.2cm in the right infraorbital region. Incision and drainage of this area was performed with an 18-gauge needle that revealed clear yellow, odorless, slightly hemorrhagic fluid. She was then placed on levofloxacin 750mg three times daily for seven days. The aspirate was sent for gram staining and bacterial culture with no growth. Over the next week, the patient showed slow improvement; however, on Day 28, she developed similar symptoms on the contralateral side with a smaller nodule. Again, incision and drainage were performed with similar results. At this time, she was placed on a methylprednisolone dose pack and trimethoprim/ sulfamethoxazole DS twice daily for seven days. The gram stain and bacterial culture showed no growth. Within several days, the patient showed improvement of the left infraorbital region, with decrease in erythema and nodule size. At Day 49, the patient was injected with hyaluronidase (150units/cc) to help facilitate the breakdown of the HA product under both infraorbital (tear trough) areas (10–15units/area). Within days, there was marked improvement in erythema and size of the nodules (Figure 3). This treatment was repeated five days later with complete resolution of the patient’s signs and symptoms. The patient recovered without any scarring or other skin changes. After six weeks, the patient was treated with Juvederm Ultra Plus without incident.
{kind=link}
CASE REPORT 3
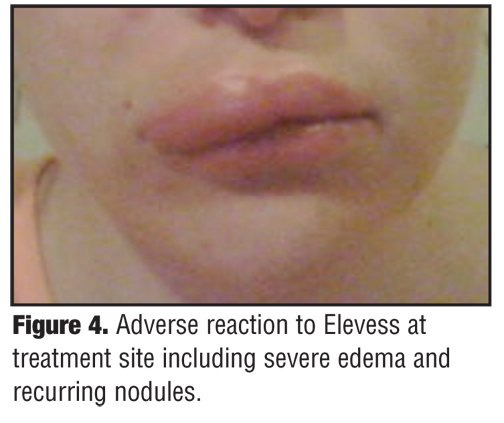
In addition to the two reported cases above, similar adverse events with Elevess were reported in a patient from a private practice (Werschler P, Assistant Clinical Professor of Medicine/Dermatology, University of Washington School of Medicine, Seattle, Washington, personal correspondence, July 20, 2009). A female was treated with Elevess to the upper and lower lips. Recurring nodules and severe edema to the treatment site (Figure 4) developed after initial swelling from the procedure had resolved. Oral steroids were administered without effect. The filler was expressed through stab incisions and the patient was started on antibiotic therapy. The patient reported that she was “squeezing puss and product” out of the affected area for two months following the attempted removal of the material (Werschler P, personal correspondence, July 20, 2009). Complete resolution of symptoms and signs was eventually achieved.
{kind=link}
DISCUSSION
Documentation of adverse reactions to injectable fillers spans all types of fillers including biodegradable (xenographs, autographs, and synthetic products) and nonbiodegradable fillers. Their associated risks do, however, vary according to the nature of the material.[7] These reactions range in severity and time after treatment and range from swelling and erythema to pain, nodule formation, pigmentation, and abscess formation.[8] Specifically, HA-based fillers are usually well-tolerated, although skin induration and injection-site reactions are not uncommon with their use.[9] Patients desiring aesthetic correction using injectable fillers should be made aware of these potential risks prior to treatment.
Side-effects common to HA-derived injectables include bruising at the injection site, redness, slight pain, and swelling. The American Society for Dermatologic Surgery (ASDS) has guidelines of care that discuss treatment of common and uncommon reactions to injectable fillers.10 The most common and minor adverse reactions are managed with the application of ice. Redness and swelling should resolve within one to two days after injection (reaction may last three days or slightly longer for lip injections). Nodules are caused by excess filler or may be the result of inflammation and/or granuloma formation. Systemic steroids, intralesional steroids, antibiotics, and/or hyaluronidase are recommended treatment for the management of nodules. Bacterial infections associated with injections are managed with appropriate antibiotics.10 Although treatment with hyaluronidase (for HA fillers) is an effective treatment, physical excision, expression, or drainage of the offending material remains the most definitive treatment of some adverse reactions to dermal fillers.[11,12]
The three cases presented show similar severe reactions to Elevess occurring within days to weeks after initial injection. The reactions took several months to resolve. All three patients had been exposed to other HA injectables without incident. Two of three used HAs after the adverse event with Elevess and experienced no negative reactions.
Each of the patients described were from separate offices and were treated by different physicians in different states at different times. This may suggest the filler carries an inherent risk and further study into the production methods of any new injectable product may be needed. The reactions only subsided after the physical removal of Elevess or its enzyme-driven degradation by hyaluronidase. It should be noted that use of hyaluronidase carries its own inherent risks including allergic reaction and it is not used to directly treat the adverse reactions, only to degrade the HA-based filler. Any effect it has on reducing adverse reactions (as noted in the above cases) would presumably be secondary to removing the filler.[13]
The formation of sterile abscesses raises questions regarding what triggered the inflammatory response. Traditionally, a normal inflammatory response must be triggered by an activation of the immune system. Such an event would involve an interaction between an immunogenic protein and the host immune cells. Inappropriate inflammatory responses, such as hypersensitivity reactions, also occur in response to invading proteins. As a glycosaminoglycan, HA is not a protein, and, accordingly, no skin testing is required prior to its use, as allergic reactions are rare.[14] We can only speculate as to the cause of the inflammatory response observed in these three cases. The results of the cultures suggest that the product was not contaminated with micro-organisms. The possibility of an allergic reaction to the product (HA) itself is unlikely, as two of these three patients received additional HA injectable filler treatments after the Elevess treatment without adverse reactions.
The product may have contained an immunogenic protein, potentially introduced through the manufacturing process. Hypersensitivity reactions to Restylane (Medicis Aesthetics Inc.) in the 1990s were thought to be related to protein contaminants. The reduction in hypersensitivity reactions from the year 2000 onward may be due, in part, to the introduction of a hyaluronic raw material with trace amounts of protein six times lower than the raw material previously used.[15]
The fact that the adverse events in two of the reported patients resolved after hyaluronidase injection suggests that the HA may be sequestering an offending protein contaminant. With the breakdown of the HA, the contaminant may become more available to clearance and subsequently the reaction subsides.
With several FDA-approved, HA-derived injectable fillers already available to patients, the potential benefits that patients may receive from the release of additional HA-derived fillers must be carefully weighed against risk. More rigorous investigation and study of all new injectable fillers may be indicated to further reduce the occurrence of adverse reactions, especially when several other well-established products are being used effectively.
Acknowledgment
The authors would like to thank Philip Werschler, MD, for Case 3 and information provided that assisted in the preparation of this report.
References
1. Andre P, Lowe N, Parc A, Clerici T, Zimmermann U. Adverse reactions to dermal fillers: a review of European experiences. J Cosmet Laser Ther. 2005;7:171–176.
2. Bachmann F, Erdmann R, Hartmann V, Wiest L, Rzany B. The spectrum of adverse reactions after treatment with injectable filler in the glabellar region: results from the injectable filler safety study. Dermatol Surg. 2009;35:1629–1634.
3. Glaich AS, Cohen JL, Goldberg LH. Injection necrosis of the glabella: protocol for prevention and treatment after use of dermal fillers. Dermatol Surg. 2006;32(2):276–281.
4. Rossner F, Rossner M, Hartmann V, et al. Decrease of reported adverse events of injectable polylactic acid after recommending an increased dilution: 8-year results from the Injectable Filler Safety Study. J Cosmet Dermatol. 2009;8(1):14–18.
5. Friedman PM, Mafong EA, Kauvar ANB, Geronemus RG. Safety data of injectable nonanimal stabilized hyaluronic acid gel for soft tissue augmentation. Dermatol Surg. 2002;28(6):491–494.
6. United States Food and Drug Administration. Center for Devices and Radiological Health. Office of Device Education. Executive Summary—Dermal Filler Devices. GPO 2008.
7. Lowe NJ, Maxwell CA, Patnaik R. Adverse reactions to dermal fillers: review. Dermatol Surg. 2005;31(11):1616–1625.
8. Zielke H, Wolber L, Wiest L, Rzany B. Risk profiles of different injectable fillers: results from the injectable filler safety study (IFS Study). Dermatol Surg. 2008;34(3):326–335.
9. DeLorenzi C, Weinberg M, Solish N, Swift A. The long-term efficacy and safety of subcutaneously injected large-particle stabilized hyaluronic acid-based gel of non-animal origin in esthetic facial contouring. Dermatol Surg. 2009;35:313–321.
10. Alam M, Gladstone H, Kramer E, et al. ASDS Guidelines of Care: Injectable Fillers. Dermatol Surg. 2008;34:S115–S148.
11. Beljaards RC, de Roos KP, Bruins FG. NewFill for skin augmentation: a new filler or failure? Dermatol Surg. 2005;31(7):772–776.
12. Lupton JR, Alster TS. Cutaneous hypersensitivity reaction to injectable hyaluronic acid gel. Dermatol Surg. 2000;26(2):135–137.
13. Rzany B, Becker-Wegerich P, Bachmann F, et al. Hyaluronidase in the correction of hyaluronic acid-based fillers: a review and a recommendation for use. J Cosmet Dermatol. 2009;8(4):317–323.
14. Andre P, Flechet ML. Angioedema after ovine hyaluronidase injection for treating hyaluronic acid overcorrection. J Cosmet Dermatol. 2008;7:136–138.
15. Friedman PM, Mafong EA, Kauvar AN, Geronemus RG. Safety data of injectable non-animal stabilized hyaluronic acid gel for soft tissue augmentation. Dermatol Surg. 2002;28:491–494.