
 by Bruna Souza Felix Bravo, MD; Julien Totti, MD; Berta Elena Alcala Gelpi, md; Stephanie Bianco de Souza, MD; and Leonardo Gonçalves Bravo, MD
by Bruna Souza Felix Bravo, MD; Julien Totti, MD; Berta Elena Alcala Gelpi, md; Stephanie Bianco de Souza, MD; and Leonardo Gonçalves Bravo, MD
Dr. B. Bravo and Dr. Gelpi are with the Institute of Dermatology of Professor Rubem David Azulay in Rio de Janeiro, Brazil. Dr. Totti de Bastos is with the Federal Hospital of Lagoa in Rio de Janeiro, Brazil. Dr. Biaco de Souza is with Gamboa Hospital in Rio de Janeiro, Brazil. Dr. L. Bravo is a full member of the Brazilian Society of Plastic Surgery and is a plastic surgeon at the Burn Center at Hospital Souza Aguiar in Rio de Janeiro, Brazil.
Abstract: Generally, the shape of women’s eyes are distinctly different in intercatal height from that in men. Ideally, in a woman, the lateral intercostal point is positioned above the medial intercostal point, which gives the eyes a cat-like appearance that culturally suggests youth and health. Because of aging and/or physiological changes, this area can be altered with the inversion of the lateral intercantal line lower than the medial intercantal line, producing a tired and/or sad looking appearance. Hyaluronic acid is a quick and safe method of elevating the lateral intercantal area of the eye. This article describes a technique for using hyaluronic acid for the treatment of scleral show.
Keywords: Scleral show, hyaluronic acid, fillers
J Clin Aesthet Dermatol. 2018;11(6):38–40
Introduction
Scleral show is an anatomical condition in which the sclera area is visibly augmented due to aging, trauma, endocrine disease, or as a result of an unsuccessful blepharoplasty.1,2 Patients with constitutional scleral show also typically have an inversion of the lateral and medial corners of the eyes, which is not considered aesthetically ideal in Italy.3
Recently, more advanced and broader use of hyaluronic acid (HA) fillers has allowed for the treatment of constitutional scleral show in a quick, noninvasive, and safe manner. This article describes the technique using HA for the treatment of scleral show.
Female Versus Male Eye Shape
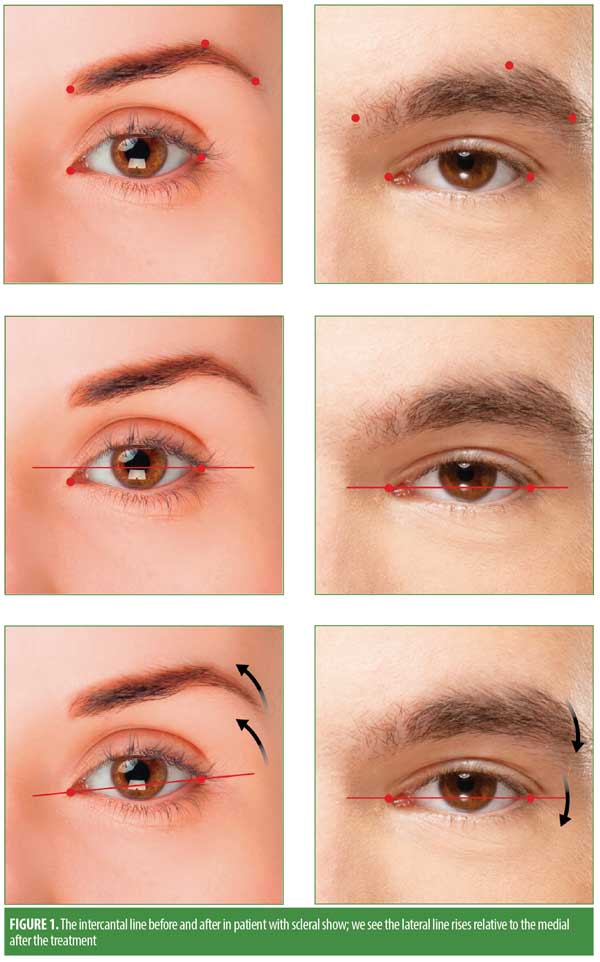
The eyelid is 700 to 800?m thick, protecting the anterior surface of the globe and maintaining the tear film, necessary for the preservation of the cornea. Typically, the open upper eyelid covers 1 to 2mm of the iris, while the open lower eyelid covers the eyeball up to the base of the iris. The so-called scleral show occurs when the eyelid fissure is increased by malocclusion of the lower eyelid or due to physiological changes.4 The appearance and dynamics of female eyes differ from male eyes. The main difference is the angle of the medial intercantal axis and the lateral axis. In women, the lateral axis is discreetly higher in relation to the medial axis, termed by the authors as a cat’s eye or an attractive eye. The female eyebrow in conjunction with the eyes has a lower medial angulation and a higher tail compared to that of the male eyebrow. The lateral third of the eyebrow has the highest arch point and coincides with the lateral limbus of the eyes. In men, these axes tend to be oriented horizontally, and the eyebrow is rectified.3 A schematic of the ideal patterns of female and male beauty is presented in Figure 1.
HA Filler for Treatment of Scleral Show
When a patient has an apparent scleral show because of constitutional or iatrogenic reasons, fillers with HA are suitable treatment options. The filling of this area is performed strategically to produce an elevation of the lateral corner of the eyelid in relation to the medial one in women. In men, the same technique can be used to rectify the eye.3 In this article, we present a technique using HA as a treatment for constitutional scleral show. The technique can also be used in patients with postblepharoplasty scleral show, though each case should be considered individually and physicians should be cautious about the greater risk of local postsurgical fibrosis.
Technique. The HA filling to treat scleral show can be performed using a 27-gauge cannula and low crosslinking HA. If the technique is done with a needle, aspiration prior to the injection of the filler is required in order to avoid intravascular injections. Asepsis should be performed with alcoholic chlorhexidine 2%, and materials should be sterile.
The technique consists of introducing a cannula in the submuscular plane using an entry point located at the lateral corner of the eye. The cannula is inserted immediately below the lateral raphe of the lower eyelid in a medial direction in the infratarsal region of the eye, with positioning of the cannula close to the inferior margin of the palpebral limbus of the eyelid. The application can be done by retroinjection, and about 0.01mL is injected in each side. HA filling can also be used in the tear trough and palpebromalar groove for better results.
Immediately after the procedure, if a small nodulation at the site of the application occurs, it should be massaged into the product.
In our practice, Juvederm Volbella® (Allergan, Dublin, Ireland) is our HA filler of choice for this procedure because it is the product with which we have the most experience; however, other low crosslinking HA products could be used. Low crosslinking HA is malleable, making local massage easy and reducing the occurence of nodules and overcorrection.
Examples scleral show correction of the lower lids are shown in Figures 2 and 3. Noteworthy improvement with elevation of the lateral corner of the eyes relative to the medial corner can be seen in the figures, yielding more attractive eyes that follow the ideal beauty standards that are recommended in the literature.4


Discussion
HA fillers have vast uses in aesthetic dermatological treatments for rejuvenation and beautification, as well as in therapeutic treatments. As noted in this paper, HA fillers can improve scleral show as well as provide elevation of the lateral corner of the eye in correspondence with the medial corner by adding volume, expanding the local tissue, and raising the lateral corner of the lower eyelid. In addition to constitutional scleral show, HA also offers therapeutic options for addressing scleral show due to acquired lesions.
The success of HA treatment for cicatricial ectropion was described by Fezza5 in a study with 15 patients, with significant correction of ectropion and no complications except for temporary bruising and Tyndall effect.5
Romero et al6, using HA for the correction of cicatricial ectropion, demonstrated partial or total improvement of aesthetic ectropion and related symptoms, such as conjunctival and corneal dryness, in 11 treated patients. The main complication observed was irregular fullness. However, the authors suggested that this treatment should be considered only for patients with surgical restrictions or those who do not want to undergo a surgical procedure. Simon and Hariri2 reported successful outcomes in two patients treated with 0.8cc of HA for the correction of ectropion, caused by traumatic injury due to thermochemical burns in one patient and following blepharoplasty in the other patient. Both patients showed improvement of the cicatricial ectropium without the need for additional surgery.2
Our experience has shown an improvement in the appearance of constitutional scleral show using this HA technique, and we believe our results are very close to that of ideal beauty standards in Italy. We have observed no adverse effects following the treatment, and the complications have been similar to those of tear-trough filling.
Possible complications related to filling with HA for the treatment of scleral show, such as bruising, overcorrection, nodulation, Tyndall effect, and ischemia (which is rare because the procedure is performed with cannula), are similar to those reported in the filling of dark circles.8
Additional research is needed to better evaluate benefits, long-term results, and safety using HA fillers for the treatment of scleral show.
References
- Loeb R. Scleral show. Aesthetic Plast Surg. 1988;12(3):165–170.
- Simon J, al Hariri AB. The role of hyaluronic acid injections in the management of cicatricial ectropion. Abstract presented at the Southern Medical Association Annual Scientific Assembly; Oct. 30–Nov. 1, 2014; Destin, FL.
- Prendergast PM. Facial proportions. In: Erian A, Shiffman MA, editors. Advanced Surgical Facial Rejuvenation. Berlin, Germany: Springer-Verlag; 2012:15–22.
- Fábio Meneghini, Paolo Biondi. Clinical Facial Analysis: Elements, Principles, and Techniques. 3rd ed. New York, NY: Springer; 2005:59–63.
- Palermo EC. Anatomia da região periorbital. Surg Cosmet Dermatol. 2013;5(3):24556.
- Fezza JP. Nonsurgical treatment of cicatricial ectropion with hyaluronic acid filler. Plast Reconstr Surg. 2008;121(3):1009–1014.
- Romero R, Sanchez-Orgaz M, Granados M, et al. Use of hyaluronic acid gel in the management of cicatricial ectropion: results and complications. Orbit. 2013;32(6): 362–365.
- Lafaille P, Benedetto A. Fillers: contraindications, side effects and precautions. J Cutan Aesthet Surg. 2010;3(1):16–19.