
Matthew A. Molenda, MD, Division of Dermatology, The Ohio State University Medical Center, Columbus, Ohio; Novie Sroa, MD, Division of Dermatology, The Ohio State University Medical Center, Columbus, Ohio; Shannon M. Campbell, DO, Division of Dermatology, Ohio University O’Bleness Hospital; Athens, Ohio; Mark A. Bechtel, MD, Division of Dermatology, The Ohio State University Medical Center, Columbus, Ohio; E. Mitch Opremcak, MD, Department of Ophthalmology, The Ohio State University Medical Center, Columbus, Ohio
Disclosure: Drs. Molenda, Sroa, Campbell, and Bechtel have no relevant conflicts of interest. Dr. Opremcak has filed a patent (PCT/US2005/040993) for this method of treating ecchymoses.
Abstract
Ecchymoses, commonly known as bruises, frequently occur after injury to the skin causes extravasation of red blood cells into interstitial tissue. This extravasation can lead to an inflammatory cascade. The case report presented details one patient who displayed rapid improvement in the pain and appearance of a partially treated bruise on her thigh after an eight-hour application of hydrogen peroxide 15% carbamide gel under occlusion. Hydrogen peroxide 15% carbamide gel may represent a novel treatment for ecchymoses. This potential new treatment for bruises needs to be studied further to detail its adverse effects, safety profile, and efficacy profile. (J Clin Aesthet Dermatol. 2010;3(11):36–38.)
Ecchymoses, commonly known as bruises, result from various insults to the skin including, but not limited to, localized trauma, bleeding disorders, scurvy, surgery, and cosmetic procedures.
They represent a final common pathway for a variety of pathophysiological processes associated with vascular permeability near the cutaneous venules or papillary dermis capillary loops.[1] The normal function of endothelial cells is to prevent large amounts of blood from egressing from the vasculature. Endothelial cell integrity can be compromised by several factors that cause damage to endothelial cells, such as direct trauma, circulating toxins in sepsis, lactic acid accumulation in hypoxia, or mechanical obstructions resulting in increased intraluminal pressure. The resultant erythrocyte extravasation from damaged capillaries into the interstitial tissue causes an inflammatory reaction.[2,3] Within a few hours after the injury, inflammation invariably causes edema, further promoting inflammation. The involved area changes in color from deep purple, to black and blue, to green, then to yellow as the hemoglobin is degraded to bilirubin.[2,4] These changes can be alarming to the patient who is not counseled to expect the possibility of bruising. The concern is mainly cosmetic and temporary because most bruises resolve with time and leave no sequelae.
Bruises can be painful and unsightly, so many methods have been tried to alleviate and minimize bruising. Therapeutic options for ecchymoses have traditionally focused on preventative measures. Depending upon existing comorbidities and risk, some patients are instructed to avoid taking aspirin, nonsteroidal anti-inflammatory drugs, and herbal medicines that may affect bleeding prior to or immediately following a procedure. The application of ice or the use of epinephrine combined with an anesthetic is commonly employed to decrease or prevent ecchymosis formation, but is not consistently effective. Corticosteroids have been the mainstay of systemic medications used to treat postoperative edema and ecchymoses.[5–7] In addition, herbal medications and vitamin derivatives have yielded mixed results in attempts to decrease facial ecchymoses. These herbal medications have been studied for their anti-inflammatory properties and include bromelains,[8] Arnica montana,[9,10] and melilotus extract.[11] One of the main treatments used to hasten the cosmetic improvement of bruises has been topical vitamin K. The mechanism of action for localized topical vitamin K application speeding up bruise resolution is unknown, as local application is not thought to significantly affect liver production of coagulation factors.[12,13] Studies by Cohen et al[12] and Shah et al[13] showed success with the use of topical vitamin K to hasten the resolution of purpura caused by pulsed dye laser (PDL). While PDL causes bruising, it has also been evaluated as a method to expedite the resolution of ecchymoses once they have formed. DeFatta et al[14] demonstrated that the PDL was effective at hastening the time for bruises to heal with little discomfort to patients.
The authors report a case in which 15% hydrogen peroxide carbamide gel minimized the discoloration and discomfort associated with bruising. When applied to the skin under occlusion with an adhesive bandage, a hydrated gel con-taining hydrogen peroxide (H2O2) 5 to 20% or carbamide peroxide (CH6N2O3, hydrogen peroxide combined with urea) gel 5 to 20% can, in the principal investigator’s experience, significantly improve the aspects of bruising that patients often find troubling.
Case presentation
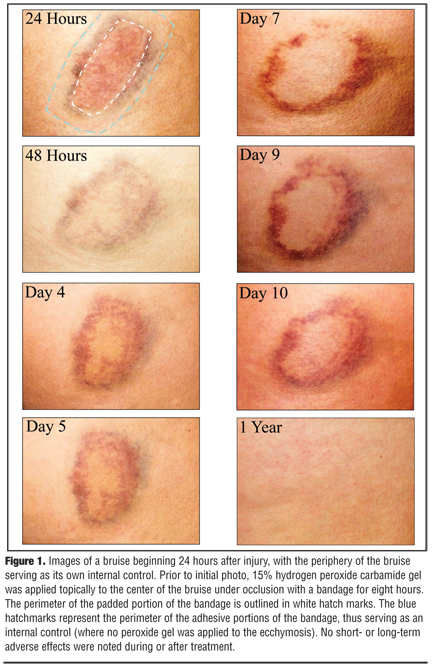
A 49-year old healthy woman was shoved into a door by her dog. A bandage with 15% hydrogen peroxide carbamide gel was placed only in the center of the bruise for an eight-hour period overnight (for one night only). The treatment was applied 12 to 18 hours after the injury. Figure 1 shows the progression of the bruise beginning 24 hours after initiation of one treatment. The bruise served as its own internal control. The top left image shows the shape of the bandage, with the white hatchmarks representing the perimeter of the padded portion of the bandage and the blue hatchmarks representing the perimeter of the adhesive portion of the bandage. In the principal investigator’s experience, patients who used peroxide gels (?20%) on their skin did not experience any irritation, dryness, or adverse effects from topical application. Most patients did report improvement in the discoloration, pain, and edema associated with their bruises. No skin bleaching was noted immediately after the bruise faded and no long-term skin bleaching resulted from this case, demonstrated by an approximately one-year post-application photo seen on the bottom right of Figure 1.
{kind=link}
DISCUSSION
While no formal studies have been conducted on the safety of peroxide gels under occlusion on bruised skin, peroxides are widely used over the counter and in the medical setting. Hydrogen peroxide 3% solution is sold over the counter as a topical antiseptic since its oxidizing properties inhibit microbial growth.[15–17] It is often sold in opaque bottles because light can lead to a more rapid degradation of hydrogen peroxide into water (H2O).[17] Carbamide peroxides are used for teeth whitening in concentrations of 5 to 20%. Most dental preparations used for teeth whitening are 10% carbamide peroxide.[15–17] Carbamide peroxide (6.5%) is also used as an over-the-counter ear wax softener, and hydrogen peroxide (5%) can be used to bleach hair by oxidizing melanin.[15]
In 1974, the United States Food and Drug Administration (FDA) released a monograph (FDA 72–104) on hydrogen peroxide detailing biochemical data and safety and toxicity studies. The FDA has set the upper limit on peroxide strength at 20% carbamide peroxide and 6% hydrogen peroxide for peroxide gel over-the-counter drugs (e.g., oral wound cleansers). At higher concentrations, there is an increased risk of side effects, such as irritation of mucous membranes or skin. According to the FDA in its Code of Federal Regulations, hydrogen peroxide is “Generally Recognized As Safe” as a bleaching agent.[18]
Hydrogen peroxide is classically thought to produce a bleaching effect by breaking light-absorbing double-bonds within color pigments.[15,16] Hydrogen peroxide is also a well-known cause of hemolysis, as there have been multiple reports of its hemolytic effects when used as a disinfectant in hemodialysis units.[19] Since a bruise is made up of red blood cells extravasated into the dermis and subcutaneous tissue, the hydrogen peroxide in this case theoretically causes localized lysis in the extravasated red blood cells. In addition, lightening of a bruise may also be due to breaking of double bonds in erythrocyte pigments. In the authors’ experience, no effect was observed on patient background pigmentation.
Additional studies are needed to evaluate the safety and efficacy of peroxide gel treatment for bruises. Additional studies could include biopsies of treated and untreated portions of bruises; placebo-controlled, blinded studies; measurement of hemoglobin before and after treatment of large bruises to demonstrate safety; evaluation of changes in skin pigmentation and integrity; evaluation of depth of penetration; and other applications for topical peroxide gels under occlusion. For example, if hydrogen peroxide gels can penetrate stratum corneum and the rest of the epidermis, they may also be able to penetrate the nail plate to treat conditions such as onychomycosis or subungual hematomas.
References
1. Jaffe FA. Petechial hemorrhages. A review of pathogenesis. Am J Forensic Med Pathol. 1994;15(3):203–207.
2. Bithell TC. Blood coagulation. In: Lee RG, ed. Wintrobe’s Clinical Haematology. Philadelphia: Lea & Febiger; 1993:566–615.
3. Byard RW, Krous HF. Petechial hemorrhages and unexpected infant death. Leg Med (Tokyo). 1999;1(4):193–197.
4. Dinehart SM, Henry L. Dietary supplements: altered coagulation and effects on bruising. Dermatol Surg. 2005;31:819–826.
5. Kara CO, Gökalan I. Effects of single-dose steroid usage on edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Plast Reconstr Surg. 1999;104(7):2213–2218.
6. Totonchi A, Guyuron B. A randomized, controlled comparison between arnica and steroids in the management of postrhinoplasty ecchymosis and edema. Plast Reconstr Surg. 2007;120(1):271–274.
7. Kargi E, Ho?nuter M, Babucçu O, et al. Effect of steroids on edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Ann Plast Surg. 2003;51(6):570–574.
8. Seltzer AP. A double-blind study of bromelains in the treatment of edema and ecchymoses following surgical and non-surgical trauma to the face. Eye Ear Nose Throat Mon. 1964;43:54–57.
9. Seeley BM, Denton AB, Ahn MS, Maas CS. Effect of homeopathic Arnica montana on bruising in face-lifts: results of a randomized, double-blind, placebo-controlled clinical trial. Arch Facial Plast Surg. 2006;8(1):54–59.
10. Alonso D, Lazarus MC, Baumann L. Effects of topical arnica gel on post-laser treatment bruises. Dermatol Surg. 2002;28(8):686–688.
11. Xu F, Zeng W, Mao X. The efficacy of melilotus extract in the management of postoperative ecchymosis and edema after simultaneous rhinoplasty and blepharoplasty. Aesth Plast Surg. 2008;32:599–603.
12. Cohen JL, Bhatia AC. The role of topical vitamin K oxide gel in the resolution of postprocedural purpura. J Drugs Dermatol. 2009;8(11):1020–1024.
13. Shah NS, Lazarus MC, Bugdodel R, et al. The effects of topical vitamin K on bruising after laser treatment. J Am Acad Dermatol. 2002;47(2):241–244.
14. DeFatta RJ, Krishna S, Williams EF. Pulsed-dye laser for treating ecchymoses after facial cosmetic procedures. Arch Facial Plast Surg. 200;11(2):99–103.
15. Hydrogen peroxide: practical, environmentally friendly and antibacterial (2007-2008). Did you know there were so many uses for hydrogen peroxide? http://www.using-hydrogen-peroxide.com/. Accessed on May 20, 2010.
16. Hydrogen peroxide. http://en.wikipedia.org/wiki/Hydrogen_ peroxide. Accessed on May 20, 2010.
17. Material Safety Data Sheet Hydrogen Peroxide (20-40%) (June 3, 2008). MSDS. http://msds.fmc.com/msds/ 100000010225-MSDS_US-E.pdf. Accessed on May 20, 2010.
18. U.S. Government Printing Office via GPO Access. Code of Federal Regulations, Title 21, Volume 6 [21CFR582.1366] FDA. Revised as of April 1, 2002.
19. Albright RK, White RP. Red blood cell susceptibility to hydrogen peroxide (H2O2) lysis in chronic hemodialysis patients. Clin Exp Dial Apheresis. 1982;6(4):223–228.