
Case Report and Literature Review
Saira B. Momin, DO; Dermatology Resident (PGY-3), Valley Hospital Medical Center, Touro University College of Osteopathic Medicine, Las Vegas, Nevada; Blakely S. Richardson, MSIV; University of North Texas Health Science Center, Fort Worth, Texas;
Michael G. Bryan, MD; Clinical Associate Professor (Dermatology), University of Nevada School of Medicine; Clinical Instructor of Dermatology, Valley Hospital Medical Center, Las Vegas Skin and Cancer Clinics, Las Vegas, Nevada;
James Q. Del Rosso, DO; Dermatology Residency Director, Valley Hospital Medical Center, Clinical Associate Professor (Dermatology), Touro University College of Osteopathic Medicine and University of Nevada School of Medicine, Las Vegas Skin and Cancer Clinics, Las Vegas, Nevada;
Narciss Mobini, MD; Associate Director of Dermatopathology, Associated Pathologists Chartered; Clinical Assistant Professor in Dermatology, Pathology, and Medicine, University of Nevada School of Medicine, Las Vegas, Nevada
Abstract
Mycetoma is a chronic and progressive subcutaneous granulomatous infection characterized by painless swelling and tumefaction, draining sinus tracts, and purulent discharge. The term eumycetoma is used to describe an infection caused by fungi, while an actinomycetoma is used to describe an infection caused by filamentous bacteria. An accurate identification of the pathogen plays a vital role in the treatment plan as well as a positive outcome for the patient. In this report, we present an elderly white female with an initial presentation of mycetoma masquerading as a squamous cell carcinoma. We also review microbiology, diagnostic modalities, and treatment for mycetoma.
(J Clin Aesthetic Dermatol. 2009;2(2):26–31)
**********************************************************************************************************************************
Mycetoma is a chronic and progressive subcutaneous granulomatous infection characterized by painless swelling and tumefaction, draining sinus tracts, and purulent discharge. This discharge contains microbial sclerotia, or grains, which may be helpful in identifying the pathogen.[1] This inflammatory disease may be caused by fungi or bacteria and is classified accordingly. The term “eumycetoma” is used to describe an infection caused by fungi, while an “actinomycetoma” is reserved for an infection caused by filamentous bacteria.[2] Multiple diagnostic modalities are available and are an essential step in the proper evaluation of a patient. Accurate identification of the pathogen plays a vital role in the treatment plan as well as patient outcomes. Without treatment, this disease may lead to tissue destruction and deformity, eventually requiring amputation.[3]
Case Report
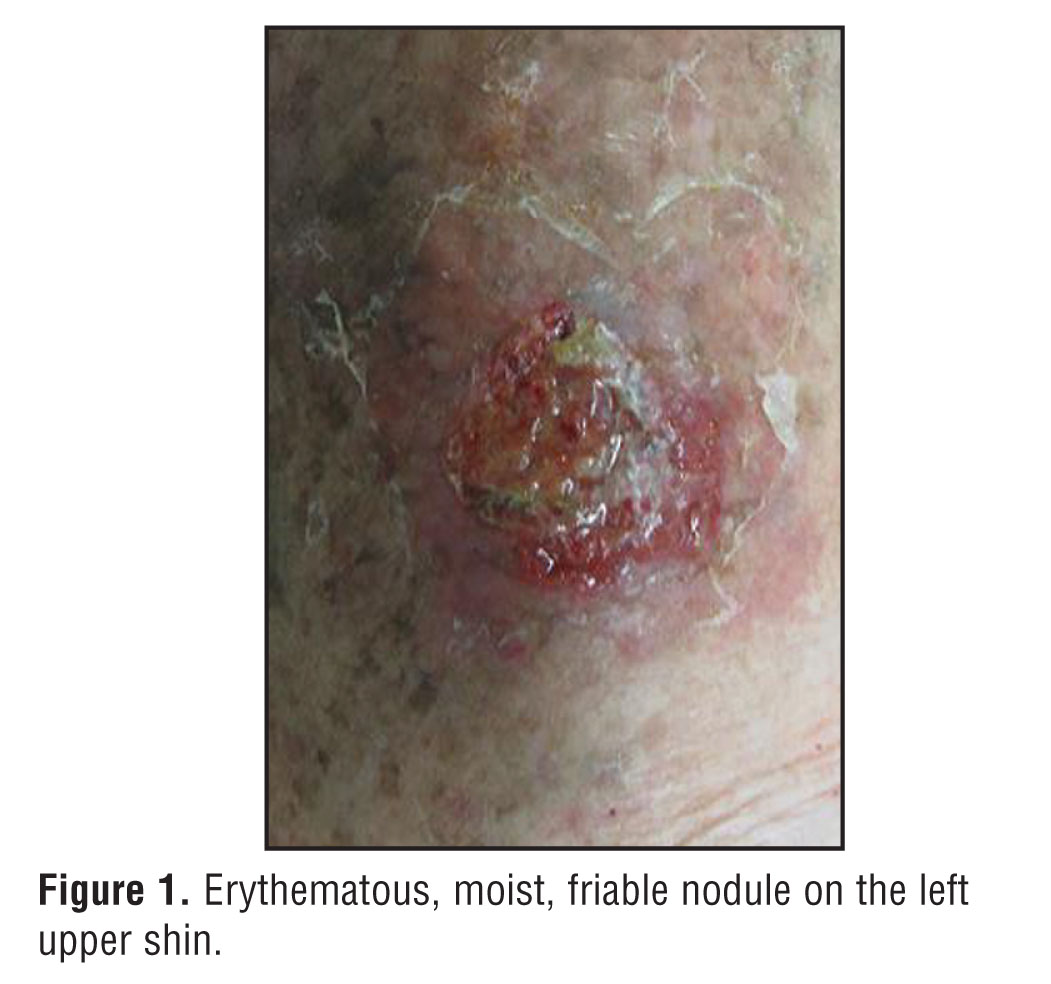
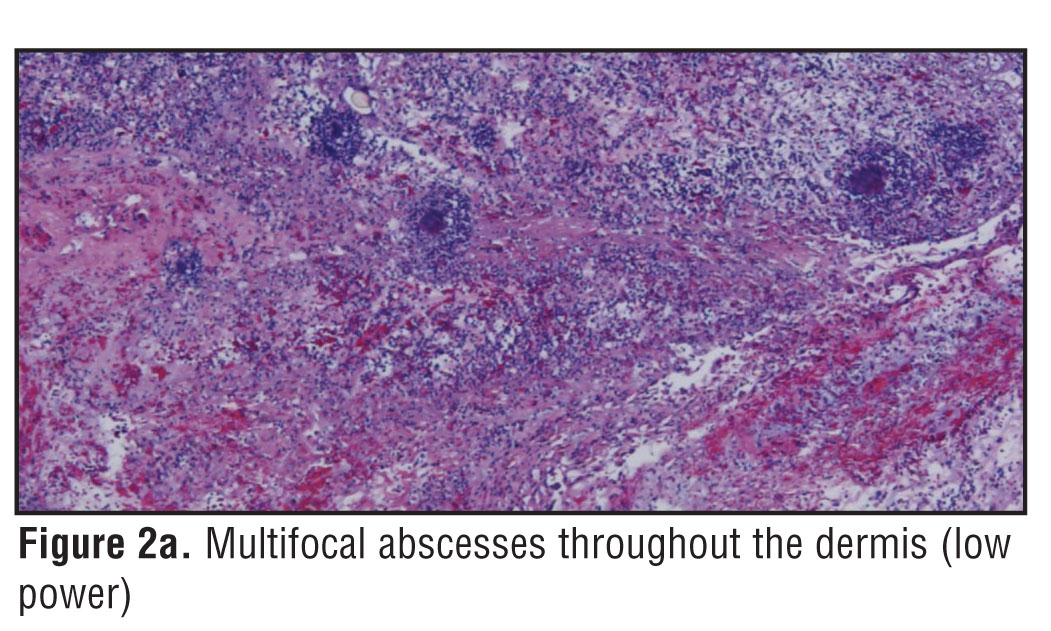
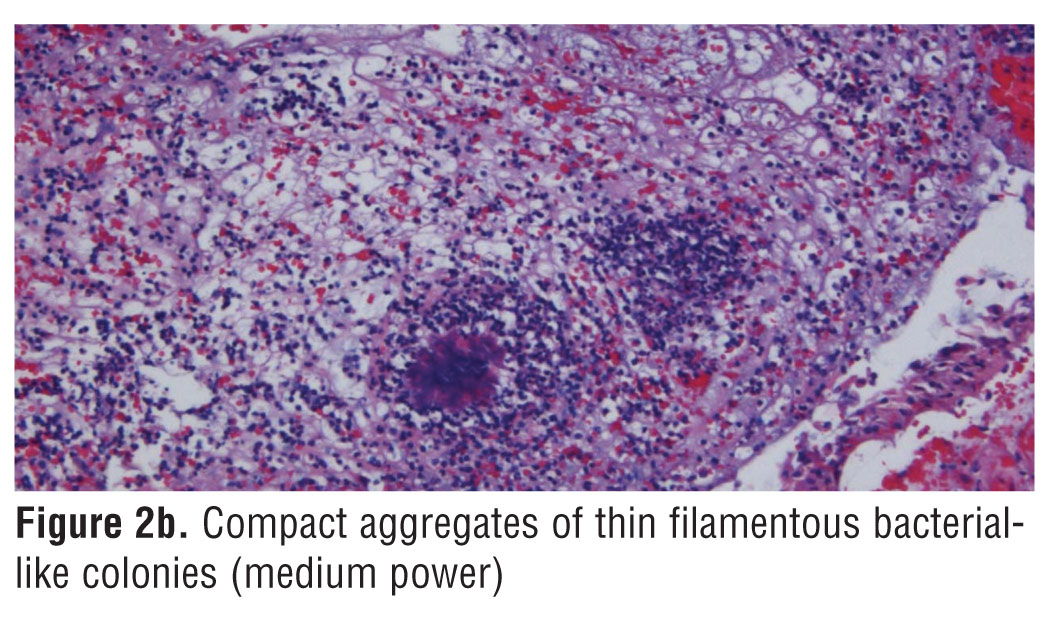
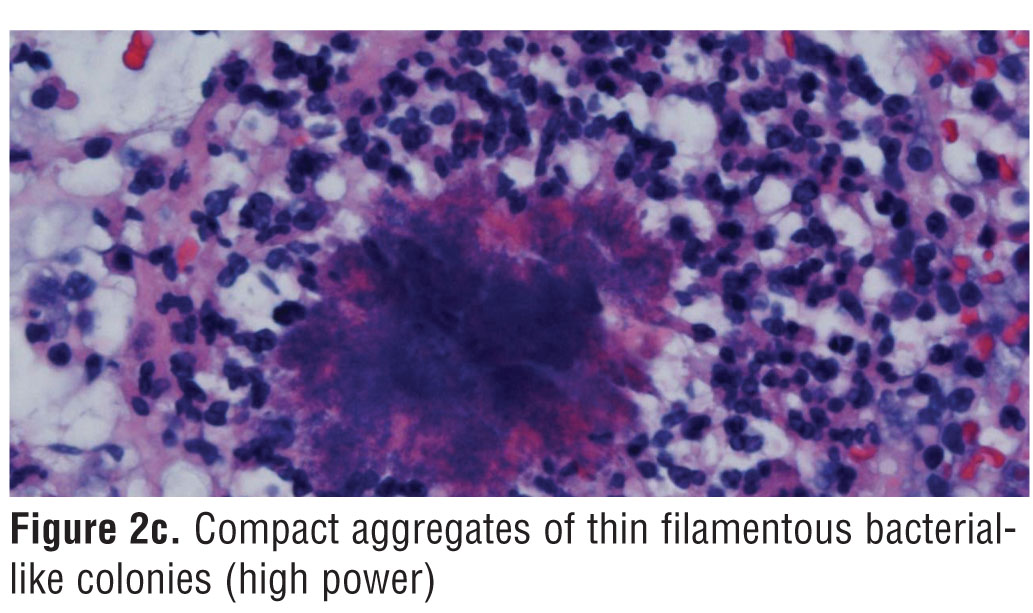
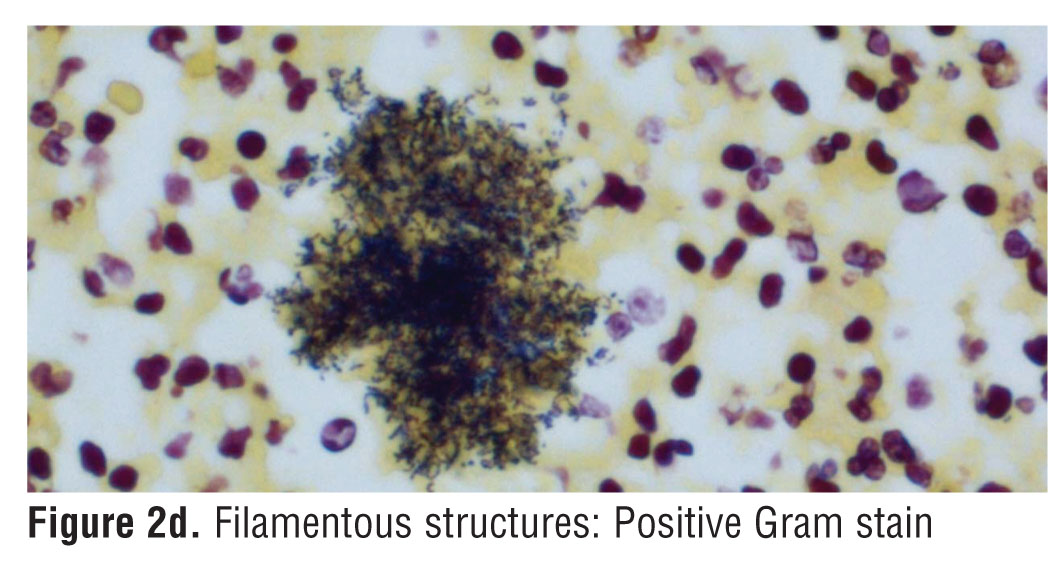
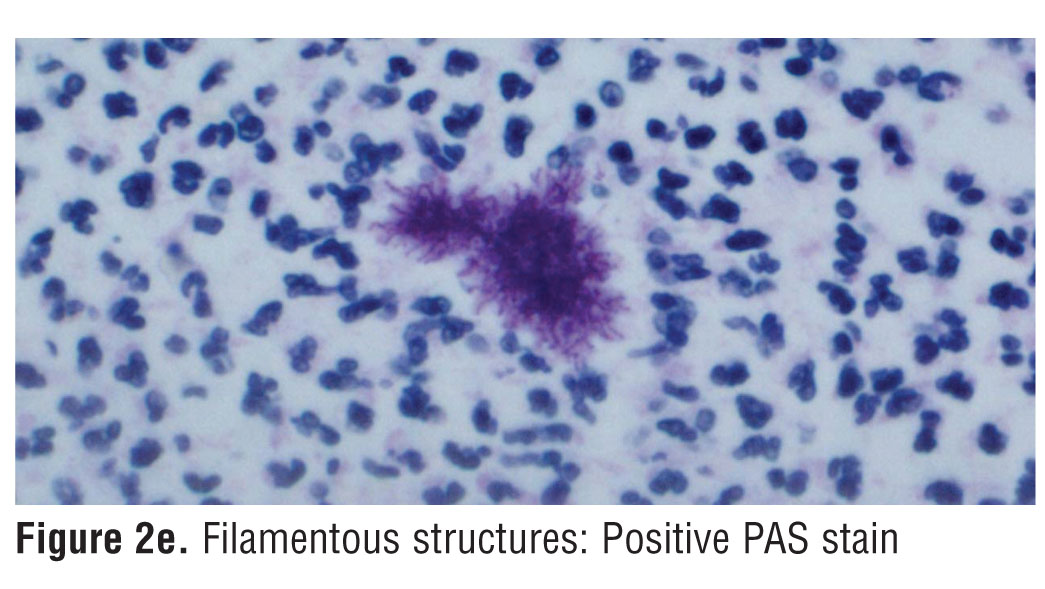
An 84-year-old Caucasian woman presented with a 3.5 x 4cm, erythematous, moist, friable nodule on the left upper shin (Figure 1). The patient stated this lesion had been “growing fast” in the last two weeks and recalled “bumping” her leg against the dresser. The patient is not an immigrant and denied any history of travel before the lesion appeared. She related a history of multiple squamous cell carcinomas (SCC) on the lower extremities. History of SCC along with the clinical presentation of the lesion gave us a high clinical suspicion of possible SCC and a biopsy was performed. Microscopic examination revealed broad ulcerated multifocal abscesses with suppurative inflammation containing numerous neutrophils and compact aggregates of thin filamentous, bacterial-like colonies surrounded by an eosinophilic border exhibiting the Splendore-Hoeppli phenomenon (Figures 2a , 2b , 2c). The filamentous structures were positive for Gram and periodic acid Schiff (PAS) stain and negative for acid-fast bacilli (AFB) stain (Figures 2d and 2e).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
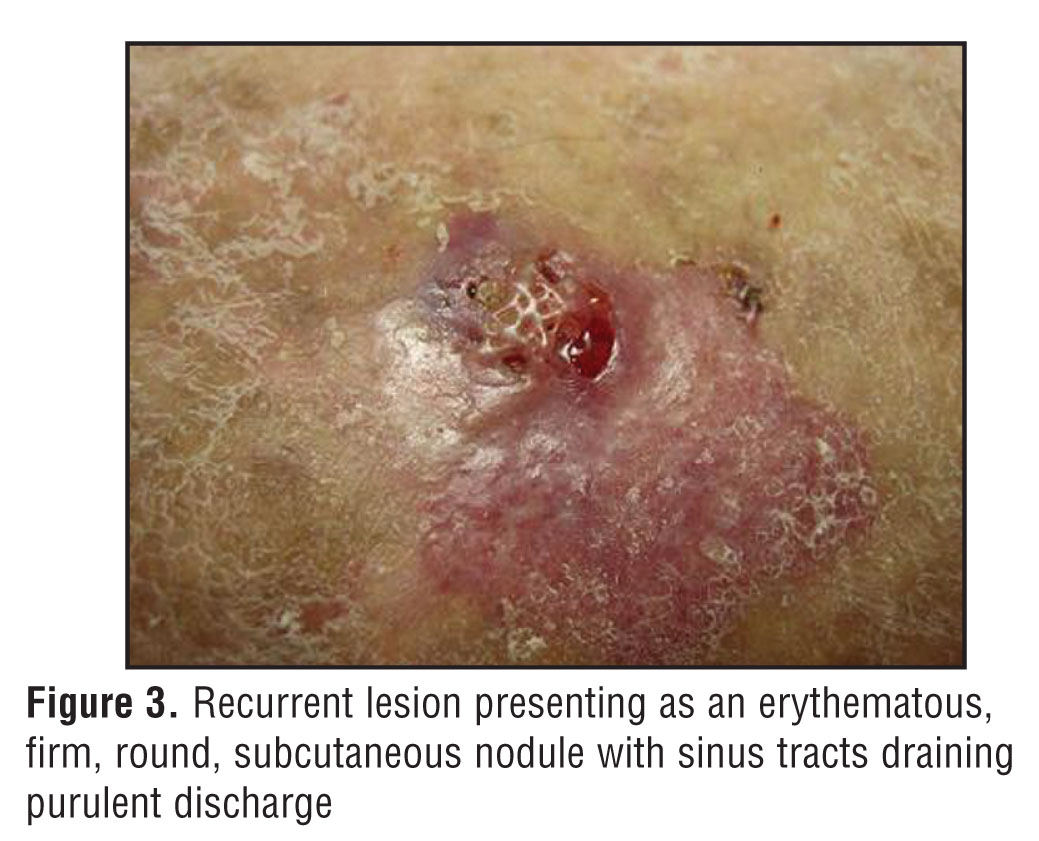
A deep saucerization biopsy was completed for bacterial and fungal cultures in an attempt to accurately identify the microorganism. There was no growth for Nocardia species. There was also no growth for anaerobic bacteria, in particular Actinomyces species. This may be due to sampling error or due to diagnosis of an early lesion since mycetomas are generally slow growing, deep, chronic, infectious processes. A diagnosis of mycetoma was made, in particular actinomycetoma, based on clinical presentation and positive staining of the filamentous bacteria. The patient was treated with trimethoprim/ sulfamethoxazole 80mg/160mg twice daily and followed up in two weeks. During the follow-up visit, she stated she had been poorly compliant and was taking her antibiotic only once a day. Although the lesion had resolved clinically, the patient was counseled to take the antibiotics as instructed. She returned to the clinic six weeks later complaining of a new growth adjacent to the resolved lesion on the left upper anterior tibial region. This recurrent lesion was more characteristic of mycetoma with the presentation of an erythematous, firm, round, subcutaneous nodule with sinus tracts draining purulent discharge containing white-colored grains (Figure 3).
{kind=link}
The recurrent lesion was sampled and sent for tissue cultures. At the time this article was submitted for publication, there had been no growth over a period of eight weeks. Although the lab was alerted to hold the cultures longer, isolation of the organism can be very difficult, especially in cases of actinomycetomas.
Discussion
Mycetomas, often referred to as Madura foot and maduramycosis, are chronic granulomatous infections of the dermal and subcutaneous tissues caused by filamentous aerobic and anaerobic bacteria (actinomycetomas), true fungi (eumycetomas), and true bacteria, such as Staphylococcus aureus and Pseudomonas species (botryomycosis).[4,5] Some authors do not recognize botryomycosis as a true mycetoma and prefer the terms “bacterial pseuodmycosis” or “granular bacteriosis.”[5] This disease is not mentioned in this discussion of mycetoma.
Epidemiology. The true incidence of mycetoma remains unknown, but it is most often found in the tropics and subtropics between the latitudes 15°S and 30°N. This so-called “mycetoma belt” includes Sudan, Nigeria, Somalia, Senegal, Middle East, India, Yemen, Mexico, Venezuela, Columbia, and Argentina as well as other locations with similar climate characteristics. These are all relatively arid regions with a short rainy season and low relative humidity.[2] Actinomycetomas are common worldwide, not just in tropical countries, and eumycetomas are especially common in equatorial Africa. Although mycetoma is not endemic within the United States, increased global travel and immigration warrants the need for mycetoma awareness and education in the medical community.[3] In the United States, it is particularly seen in the south.[4]
Tumefaction, draining sinuses, and presence of grains in the pus or tissues are hallmarks of mycetoma.[6] Mycetoma is more common in people who have frequent and direct contact with field environments or outdoor activities. This includes farmers, field laborers, and herdsmen. Males are affected more often than females with the ratio being 3.7 to 1. This disease usually affects adults between 20 and 40 years of age, but children and elderly may also be affected in endemic regions.[4] During pregnancy, mycetoma may become more active and aggressive. This may be due to changes in hormonal levels or due to the decreased immune response during pregnancy.[7] A study by Mendez-Tovar et al suggests that progesterone may actually inhibit the growth of certain organisms, which may explain the higher prevalence in men.[8]
Microbiology. Eumycetomas are caused by several pathogens in different parts of the world. Acremonium species and Madurella grisea are common causative organisms of eumycetomas in Brazil, Madurella mycetomatis in India and Africa, and Pseudallescheria boydii in North America.[4] Species of the genera Fusarium and Leptoshaeria also cause eumycetoma.[9] Approximately 60 percent of mycetomas are of actinomycotic origin worldwide. Actinomycetomas are caused either by endogenous anaerobic bacteria, such as Actinomyces israellii and Actinomyces bovis, or by aerobic bacteria, such as Actinomadura species, Nocardia brasiliensis, and Streptomyces species.[4] Actinomycetes are the principal etiologic agent in Mexico, accounting for approximately 98 percent of the cases, with N. brasiliensis being identified as the cause in 86 percent of the infections.[9] There is strong geographic variation in the distribution of the infecting bacteria. Actinomadura pelletieri is more common in regions with more rainfall while N. brasiliensis and Streptomyces somaliensis predominate in dry, desert areas.[9]
The causative organisms are usually present in the soil or plant matter. Traumatic inoculation of the subcutaneous tissue by sharp objects, such as thorns, splinters, or sharp rocks has been proposed as the precipitating event of mycetoma formation. This theory is under debate as some affected patients do not report a primary injury at the infection site. In endemic areas where people are commonly barefoot and work outdoors, infection rates are expected to be higher than what has been reported. It has often proved difficult to isolate these organisms from the soil. Therefore, it has been proposed that the presence of an intermediate host may be important to the pathogenesis of this disease.[2]
Clinical presentation. Mycetoma usually presents unilaterally, with the foot being the most common site, followed by hands, legs, and less frequently, knees, arms, head and neck, thigh, and perineum.[4] However, any body part may be affected.[10] The initial presentation is characterized by painless and slowly progressive subcutaneous swelling sometimes preceded by a history of trauma. The initial site is usually firm and round, but may also be soft, lobulated, or cystic. Actinomycetomas progress more rapidly than eumycetomas. In actinomycetoma, the lesion is more inflammatory, more destructive, and may be invasive to bone at an earlier period. In eumycetoma, the lesion grows slower with clearly defined margins, is usually encapsulated for a long period of time, and typically presents with more fibrosis.[4] Multiple secondary nodules develop creating draining sinus tracts with serous, serosanguinous, or purulent discharge. Some of these sinus tracts heal over while new adjacent sinuses open creating a labyrinth of deep sterile abscesses. During the active phase of disease, these sinuses discharge grains.[2,4]
Mycetoma is typically painless in nature. It has even been proposed that the mycetoma may produce anesthetic substances within the lesion. Painful lesions may be explained by expansion into the bone or a secondary infection.[2] Skin changes may also include local hyperhidrosis confined to the lesion and the surrounding skin. The overlying skin is usually darker, but is sometimes hypopigmented. There is typically an absence of trophic changes, which may be due to the adequate blood supply within the myctetoma.[3]
Regional lymphadenopathy is common and may be due to secondary bacterial infection, lymphatic spread of the mycetoma, or immune complex deposition as part of the local immune response to infection.[3,4] Continual lymphatic spread is rarely reported and found in only 1 to 3 percent of cases. Lymphatic spread is more common in actinomycetoma than in eumycetoma and may be facilitated by inadequate surgical excision.[3] The organism multiplies in the subcutaneous tissue forming colonies that spread along fascial planes involving the skin, subcutaneous fat, and underlying structures. If left untreated, abscesses may extend into the bone, causing small cavities to develop leading to osseous destruction. Bony involvement may be extensive resulting in deformity and disability and may be fatal if the skull is affected. Madurella species only causes a focal and restricted bone lesion while Actinomadura species usually leads to massive bone destruction. N. brasiliensis may erode the vertical bodies and invade the central nervous system (CNS).[6] In rare cases and late in the disease, nerves and tendons may become involved.[2,3,4]
Differential diagnosis. The differential diagnosis includes other subcutaneous mycoses, such as sporotrichosis, chromoblastomycosis, phaeohyphomycosis, and hyalohyphomycosis. Subcutaneous mycoses occur as limited focal disease in immunocompetent individuals, but may disseminate widely in the immunocompromised population.[11] HIV patients can present with destructive patterns of clinical lesions and pulmonary dissemination with chronic osteomyelitis and severe disability.[4] Many tumors, such as SCC, lipoma, fibroma, fibrolipoma, sarcoma, and foreign body granulomas, may resemble mycetoma clinically. Osteogenic sarcoma, osteoclastoma, chronic osteomyelitis, and tuberculosis involving the bone share radiologic features consistent with advanced osseous mycetoma.[2]
Diagnosis. There are many different modalities used to diagnose mycetoma. The most definite modality relies directly on the examination of grains, looking at color and texture, microscopic examination for hyphae or filaments, and isolation of the etiologic organism.[4,12] Histopathologic examination reveals three types of tissue reactions. Type I reaction involves grains surrounded by a layer of polymorphonuclear leukocytes with the innermost neutrophils closely attached to the surface of the grain or sometimes invading the substance of the grain. Outside this layer of cells are macrophages, lymphocytes, plasma cells, and few neutrophils in granulation tissue. Layers of fibrin surround capillaries and venules and the outermost layer of the lesion contains fibrous tissue. In Type II reaction, most of the neutrophils are replaced by macrophages and multinucleated giant cells engulfing grain materials. Well-organized, epithelioid granulomas containing Langerhans giant cells are seen in Type III reaction.[3] Identification of the grains from discharge may help reveal the causative organism.[12]
A sample of purulent discharge from an open sinus or deep surgical biopsy taken from a soft or fluctuant area containing grains must be obtained. Biopsies without grains are not suitable for culture. A variety of stains including 20-percent potassium hydroxide (KOH), PAS, Gomori’s methenamine silver (GMS), or Gram stain (Brown-Brenn), aids in the visualization of grains and fungal filaments.[13] Grains from eumycetomas are also larger than those of actinomycetomas. Actinomycotic grains typically have Gram-negative centers with fine and delicate branched Gram-positive filaments about 1µm in diameter, while eumycetomas are usually seen as a mass of Gram-negative septate hyphae embedded in intercellular cement with wider filaments greater than 1µm in diameter.[3,4] P. boydii and Acremonium species commonly have white grains while black grains are more characteristic of M. mycetomatis.[3,4,15] Red grains are produced by A. pelletierii. Among the light grains, Actinomadura madurae are the largest, measuring up to 5mm in diameter, and produce white colonies.[3,4,6,9,15] S. somaliensis produce yellow-to-brown colored grains.[9] Nocardia species and Actinomyces species produce white-to-yellow colored grains.[3,15]
Although diagnosis can be suggested by clinical presentation and histology, a definitive diagnosis usually requires a positive tissue culture and identification of the etiologic agent. Isolation of the organism may be difficult, especially in the case of actinomycetomas. Grains are cultured onto media, such as Sabouraud and mycobiotic agar, to isolate fungi and blood agar to isolate bacteria. Isolation of the organism is cumbersome due to strict growth requirements, secondary infection, contamination of specimens, and the lack of viable organisms in chronic lesions.[3,12] In the absence of a positive culture, diagnosis may have to rely on clinicopathologic correlation along with the use of special stains as demonstrated by our case.
Recent molecular studies, such as polymerase chain reaction, enzyme linked immunosorbent assay, and immunoassays may be useful when repeated cultures are negative. These tests may provide better identification and detection of the disease. However, due to cross reactivity with bacterial infections, such as tuberculosis and leprosy, along with the limited availability of these specialized tests and lack of clinical data, further studies and investigations are needed.[3,4,14]
Imaging studies are useful for defining the extent of the disease. Early lesions resemble soft tissue granuloma, which presents as a dense shadow or as scattered, multiple, soft-tissue shadows on x-ray.[4] As the disease progresses, plain films show lytic lesions, sclerosis, and evidence of bone remodeling similar to findings in chronic osteomyelitis.[15] There may be a variable amount of periosteal reaction, which may be indistinguishable from osteogenic sarcoma.[2]
The mycetoma grains, their capsules, and granulomas have characteristic ultrasonographic appearances.[2] According to Fahal et al,[16] ultrasound could be used to differentiate eumycetoma from actinomycetoma. In eumycetoma, the grains produce numerous, sharp, hyper-reflective echoes, and there are single or multiple thick-walled cavities with no acoustic enhancement. In actinomycetoma, the findings are similar but the hyper-reflective echoes are fine, closely aggregated, and commonly settle at the bottom of the cavities.[16]
Mycotic mycetoma may also be accurately diagnosed by fine needle aspiration cytology, which is a simple, inexpensive, and rapid technique when there is a high index of suspicion. Fine needle aspiration cytology smears allow the visualization of the characteristic histopathologic changes. This includes the polymorphous inflammatory cells intermixed with grains, neutrophils, lymphocytes, plasma cells, histiocytes, macrophages, and foreign body giant cells. Special stains and culture studies are helpful in confirmation of diagnosis and species identification.[17]
Computed tomography (CT) has been shown to be more sensitive in detecting early bone changes when compared with magnetic resonance imaging (MRI).[3] However, Czechowski et al reported it was not possible to differentiate between eumycetoma and actinomycetoma radiologically.[18]
Treatment of eumycetoma. Greater than half of eumycetoma cases treated with an oral imidazole (i.e., ketoconazole) or triazole (i.e., itraconazole) respond well to treatment, particularly in those cases where the infection is limited to the subcutaneous tissue in an immunocompetent patient. In some patients, ketoconazole (400mg/day), itraconazole (300–400mg/day), amphotericin B (0.5–1.25mg/kg/day), and terbinafine (500–1000mg/day) have been reported to be effective for eumycetoma.[4,9] Treatment must usually be continued for up to several months to years to be effective. It is recommended that patients undergo liver function testing before and during treatment due to the potential hepatotoxicity associated with some of these oral antifungal agents, such as ketoconazole, itraconazole, and terbinafine, especially due to the need for chronic administration.[4] Development of side effects, cost of medical treatment over the long duration of therapy, and likelihood of poor patient compliance with long-term use of medication often mitigate successful treatment.[9]
Some authors consider surgery as the most acceptable line of treatment for eumycetoma. Surgical treatment options include aggressive surgical excision, debulking surgery, or amputation in advanced disease.[4] It is universally accepted that medical therapy is started before surgery and continued postoperatively to avoid recurrence.[4,9] Great care must be taken not to rupture the mycetoma capsule during surgery which may lead to contamination of the operative field.[4]
The most important criterion for cure is the clinical resolution of the lesions with the disappearance of the subcutaneous mass, healing of the sinuses, and return of the skin to normal along with other important criteria, such as negative serologic, radiologic, and ultrasonic findings.[4]
Treatment of actinomycetoma. Unlike eumycetes, actinomycetes have better response to medical treatment with antibiotics and other chemotherapeutic agents.[3,4] Medical treatment is useful in every stage of actinomycetoma, including advanced disease.[4] Mahgoub described the efficacy of cotrimoxazole (trimethoprim-sulfamethoxazole), dapsone, streptomycin, sulfadoxine/ pyrimethamine, and rifampin. He also evaluated efficacy with several combinations and found cotrimoxazole plus streptomycin to have the best results.[19] Due to high-drug resistance among these organisms, combination therapy is recommended over single-drug treatment.[3,4] The most common drug regimen includes streptomycin sulfate (14mg/kg/day) intramuscularly for four weeks, which is then given on alternate days with dapsone in a dose of 1.5mg/kg twice daily.[3,4] If this regimen is unsuccessful after a few months or if there are persistent side effects, dapsone is replaced by cotrimoxazole (14mg/kg twice daily) or rifampin (15–20mg/kg/day).[3,4] The reported cure rate varies from 60 to 90 percent, and the mean duration of the treatment is greater than one year. An incomplete course of medical treatment increases the rate of recurrence.[3,4] Other antibiotics that have been used effectively for actinomycetoma include amikacin, linezolid, amoxicillin/clavulanic acid, and imipenem.[3,9] Ramam et al described efficacy in patients that were initially placed on penicillin, gentamicin, and trimethoprim/sulfamethoxazole, then switched to maintenance treatment with amoxicillin and trimethoprim/sulfamethoxazole.[3,20] Trimethoprim/ sulfamethoxazole has been used with success in the treatment of mycetoma caused by Nocardia spp, and penicillin has been used in cases of actinomycetoma caused by Actinomyces species. However, long-term treatment is often necessary.[18,21,22] For limited clinical disease that is usually seen in the United States, trimethoprim/ sulfamethoxazole and penicillin are effective for treatment of actinomycetomas in compliant patients. Overall, the response to particular regimens of antibacterials varies among individuals with actinomycetoma, and too few trials have been performed to allow for differentiation of the most efficacious antibacterial combination for medical treatment.[3]
Cases of actinomycetoma requiring surgery include those resistant to medical therapy or with bony involvement that do not respond to repeated, long-term, conservative treatment.[3,4] A margin of healthy tissue should always be excised with the lesion because actinomycetomas have ill-defined borders.[3,4] Medical treatment should be given or continued pre- and postoperatively, as it facilitates the success of surgery, accelerates healing, and reduces the chance of relapse.[4]
Conclusion
In conclusion, while mycetoma may not be endemic in the United States, it is important to include it in the differential diagnosis when subcutaneous ulcerated nodules on the lower extremities are seen especially if there is discharge. A deep biopsy containing subcutaneous tissue with grains is needed for tissue culture to help accurately identify the causative organism. As it may be very difficult to isolate the organism, diagnosis may have to rely on clinical and pathologic presentation along with the use of special stains and the assistance of a dermatopathologist. Several therapeutic options are available, including both medical and surgical approaches. Most importantly, patient compliance is necessary for successful treatment and to prevent recurrences.
References
1. Ahmed AOA, van de Sande WWJ, Ahmed F, et al. Management of mycetoma: major challenge in tropical mycoses with limited international recognition. Curr Opin Infect Dis. 2007;20(2):146–151.
2. Fahal AH. Mycetoma: a thorn in the flesh. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2004;98(1):3–11.
3. Lichon V, Khachemoune A. Mycetoma: a review. Am J Clin Dermatol. 2006;7(5):315–321.
4. Lupi O, Tyring SK, McGinnis MR. Tropical dermatology: fungal tropical diseases. J Am Acad Dermatol. 2005;53: 931–951.
5. Picou K, Batres E, Jarratt M. Botryomycosis: a bacterial cause of mycetoma. Arch Dermatol. 1979;115:609–610.
6. Zaias N, Taplin D, Rebell G. Mycetoma. Arch Dermatol. 1969;99:215–225.
7. Fahal AH, Suliman SH. The clinical presentation of mycetoma. Sudan Med J. 1994;32:46–65.
8. Khatri ML, Al-Halali HM, Fouad KM. Mycetoma in Yemen: clinicoepidemologic and histopathologic study. Int J Dermatol. 2002;41(9):586–593.
9. Welsh O, Vera-Cabrera L, Salinas-Carmona MC. Mycetoma. Clinics in Dermatol. 2007;25:195–202.
10. Ahmed W, van Leeuwen A, Fahal W, et al. Mycetoma caused by Madurella mycetomatis: a neglected infectious burden. The Lancet Infect Dis. 2004;4(9):566A–574A.
11. Koga T, Matsuda T, Matsumoto T, Furue M. Therapeutic approaches to subcutaneous mycoses. Am J Clin Dermatol. 2003;4(8):537–543.
12. Liu A, Maender JL, Coleman N, et al. Actinomycetoma with negative culture: a therapeutic challenge. Dermatol Online J. 2008;14(4):1–8.
13. Pang KR, Wu JJ, Huang DB, Tyring SK. Subcutaneous fungal infections. Dermatol Ther. 2007;20(3):157.
14. Ahmed AOA, Abugroun EL, Sir AM. Unexpected high prevalence of secondary bacterial infection in patients with mycetoma (letter). J Clin Microbiol. 1998;36(3):850–851.
15. Ispoglou SS, Zormpala A, Androulaki A, Sipsas NV. Madura foot due to Actinomadura madurae imaging appearance. Clinical Imaging. 2003;27(4):233–235.
16. Fahal AH, Sheik HE, Homeida MM, et al. Ultrasonographic imaging of mycetoma. Br J Surg. 1997;84(8):1120–1122.
17. Gabhane SK, Gangane N, Anshu. Cytodiagnosis of eumycotic mycetoma: a case report. Acta Cytol. 2008;52(3):354–356.
18. Czechowski J, Nork M, Haas D, et al. MR and other imaging methods in the investigation of mycetomas. Acta Radiol. 2001;42(1):24–26.
19. Mahgoub ES. Medical management of mycetoma. Bull World Health Organ. 1976;54(3):303–310.
20. Ramam M, Garg T, D’Souza P, et al. A two-step schedule for the treatment of actinomycotic mycetomas. Acta Derm Venereol. 2000;80(5):378–380.
21. Nitidandhaprabhas P, Sittapairochana D. Treatment of nocardial mycetoma with trimethoprim and sulfamethoxazole. Arch Dermatol. 1975;111:1345–1348.
22. Warren NG. Actinomycosis, nocardiosis, and actinomycetoma. Dermatol Clin. 1996;14(1):85–95.