
Magalys Vitiello, MD, Clinical Dermatology Research Fellow, Florida Academic Dermatology Center/University of Miami Hospital, Miami, Florida; Begoña Echeverria, MD, Dermatology Resident (PGY-3 ), Instituto Valenciano de Oncologia, Valencia, Spain; Paolo Romanelli, MD, Associate Professor, Miller School of Medicine, University of Miami Department of Dermatology and Cutaneous Surgery, Miami, Florida; Adriana Abuchar, MD, Clinical Dermatology Research Fellow, Florida Academic Dermatology Center/University of Miami Hospital, Miami, Florida; Francisco Kerdel, BSc, MBBS, Director of Dermatology Inpatient Service, Florida Academic Dermatology Center/University of Miami Hospital, Miami, Florida
Disclosure: Drs. Vitiello, Echeverria, Romanelli, and Abuchar report no relevant conflicts of interest. Dr. Kerdel has received grants, participated in advisory boards, and is a speaker for: Abbott, Amgen, Wyeth, Astellas, Centocor, Genentech, Stiefel, Eisai, Merck, and Novartis.
Abstract
Keratoacanthomas are rapidly growing, keratinizing, epithelial neoplasms that tend to spontaneously involute and are rarely multiple or eruptive. There is still disagreement on whether or not this condition is a malignancy or a benign epidermal neoplasm; nevertheless, its appearance on tattoos has been reported in rare instances. When waiting for spontaneous involution is not an option, surgery is the preferred treatment. Other therapeutic modalities used for the treatment of this condition include radiotherapy; cryotherapy; laser therapy; and multiple intralesional, topical, and systemic agents. The authors report a patient who developed multiple, eruptive keratoacanthomas in the red ink portions of a tattoo and was successfully treated with acitretin.
(J Clin Aesthetic Dermatol. 2010;3(7):54–55.)
Keratoacanthomas (KAs) are squamous cell neoplasms of unknown origin that grow rapidly and may spontaneously regress without intervention after 4 to 6 months. They usually appear as isolated, single lesions over sun-exposed areas, but rarely can be multiple and eruptive (KA of Grzybowski and Ferguson Smith KA).[1,2] KAs are neoplasms composed of strands and nodules of atypical squamous cells with mitotic activity and cellular atypia that become less prominent as the neoplasms progress into the maturation phase. Additionally, fibrosis, granulation tissue formation, and a mononuclear inflammatory infiltrate are seen in the involution stage.[3] Several forms of KA have been described including trauma-induced KA and those following the injection of ink solids through the epidermis into the dermis. The characteristic reaction associated with KAs resembles a pseudoepitheliomatous hyperplasia.[4]
Case report
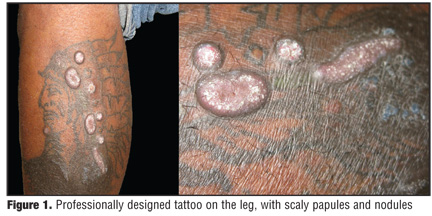
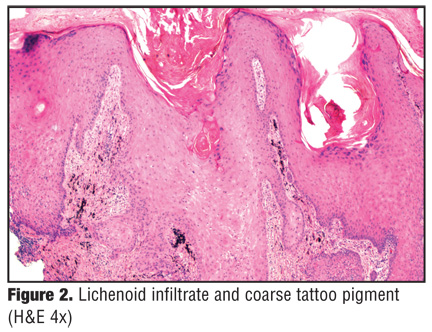
A 39-year-old African-American man presented to the authors’ practice with a two-month history of nodular lesions on his left leg associated with an itching and burning sensation. These lesions appeared over the same area in which the patient received a tattoo three months earlier. Upon physical exam, on the lateral aspect of the left leg, there were several red scaly plaques, papules, and dome-shaped, indurated nodules with crateriform surface within the red pigment of the professionally designed tattoo (Figure 1). Since the lesions clinically resembled an atypical mycobacterial infection, empirical clarithromycin 500mg twice daily and doxycycline 100mg twice daily were started. A biopsy was performed that showed marked pseudoepitheliomatous epidermal hyperplasia with chronic and focal granulomatous reaction of papillary dermis associated with mild inflammatory changes and lichenification (Figure 2 and Figure 3). Tissue periodic acid-Schiff and Fite stains were negative for concomitant micro-organisms. Polarization was negative for refractile material. After correlation of clinical and histopathological findings, the diagnosis of keratoacanthoma arising in a tattoo reaction was made and the patient was started on acitretin 25mg once daily.
{kind=link}
{kind=link}
{kind=link}
Discussion
There are several reports of keratoacanthomas arising from a tattoo, and in 82 percent of the cases, red ink was the main offending substance. It is hypothesized that the skin tries to eliminate the foreign body by creating granulomas or lysing the offender via a cytotoxic or humoral immune response. Furthermore, the finding of red ink alignment along the borders of the KA and the presence of ink in the overlying keratin suggests transepidermal elimination of the pigment via adnexal hyperplasia. These processes contribute to the formation of KA and some authors consider this a reactive rather than a neoplastic condition. Surgery is the primary treatment for lesions not involuting on their own or not responding to medical treatment by 6 to 8 weeks. Surgical excision should include 4 to 6mm margins and close follow up since KA is sometimes difficult to differentiate from squamous cell carcinoma.[2–4] In older patients who are not surgical candidates, radiation therapy may be useful. Laser therapy and cryotherapy can be used for small lesions located in difficult areas. Intralesional agents have also shown good responses and include methotrexate, bleomycin, 5-fluorouracil, steroids, and topical agents, such as imiquimod alone or in combination with retinoic acid. Other systemic therapies include cyclo-phosphamide and retinoids. Inhibition of keratinization seems to be the mechanism by which the retinoids work for KA. Acitretin, a metabolite of etretinate that inhibits the growth of atypical keratinocytes, used in a dose of 25mg once daily is the preferred treatment for resistant lesions and for patients in whom surgery or radiation therapy can cause serious disfiguration or functional impairment.[3,5–7] In the patient described in this case, the characteristics of the lesions were not indicative of malignancy; they were eruptive in nature, associated with a specific offender (red ink), and displayed classic KA histopathology. On the other hand, since the patient was symptomatic and the authors were presented with the aesthetic challenge of having multiple lesions excised in such a small surface area, surgical treatment was not ideal. Waiting for spontaneous regression was also rejected as an option. Acitretin was well tolerated and appeared to be effective, as the patient’s lesions diminished to half their size after four weeks of treatment. Following up on KA cases for recurrence and possible malignant transformation is important.
References
1. Fitzpatrick T, Eisen A, Wolff K, et al, eds. Keratoacanthoma. In: Dermatology in General Medicine. 4th ed. New York, NY: McGraw-Hill; 1993:848–855.
2. Kluger N, Minier-Thoumin C, Plantier F. Keratoacanthoma occurring within the red dye of tattoo. J Cutan Pathol. 2008;35:504–507.
3. Dos Santos Gon A, Minelli L, Garbosa Meissner MC. Keratoacanthoma in a tattoo. Dermatology Online Journal. 2009;15(7):9.
4. Fraga GR, Prossick TA. Tattoo-associated keratoacanthomas: a series of 8 patients with 11 keratoacanthomas. J Cutan Pathol. 2010;37:85–90.
5. Rosenblum GA. Multiple palmar keratoacanthomas treated with acitretin. J Drugs Dermatol. 2006;5:1006–1009.
6. Kleinerman R, Greenspan A, Hale EK. Case reports: Mohs micrographic surgery for an unusual case of keratoacanthoma arising from a longstanding tattoo. J Drugs Dermatol. 2007;6:931–932.
7. Goldenberg G, Patel S, Patel MJ et al. Eruptive squamous cell carcinomas, keratoacanthoma type, arising in a multicolor tattoo. J Cutan Pathol. 2008;35:62–64.