
J Clin Aesthet Dermatol. 2019;12(6):27–28
 by Brooke Vasicek, MD; William Adams, PhD; Laryn Steadman, BFA; Jeave Reserva, MD; and James Swan, MD
by Brooke Vasicek, MD; William Adams, PhD; Laryn Steadman, BFA; Jeave Reserva, MD; and James Swan, MD
Drs. Vasicek, Reserva, and Swan are with the Division of Dermatology at the Loyola University Medical Center in Hines, Illinois. Dr. Adams is with the Biostatistics Core, Health Sciences Division at the Loyola University Chicago in Chicago, Illinois. Ms. Steadman is with the Indiana University School of Medicine in Indianapolis, Indiana.
FUNDING: No funding was provided for this study.
DISCLOSURES: The authors have no conflicts of interest relevant to the content of this article.
ABSTRACT: Introduction.Isotretinoin treatment has been linked to flares of severe acne, which can be managed by the coadministration of systemic corticosteroids or prevented by beginning with a low dose of isotretinoin. To our knowledge, there are no estimates in the literature on the frequency of coprescription of isotretinoin and systemic corticosteroids.
Objectives.We sought to quantify the estimated frequency of coprescription of isotretinoin and systemic corticosteroids and assess trends of the use of isotretinoin with systemic corticosteroids for acne as they relate to age, sex, race, insurance, and provider specialty.
Methods. Data from the National Ambulatory Medical Care Survey (NAMCS) from 2003 to 2015, National Hospital Ambulatory Medical Care Survey Hospital Outpatient Departments (NHAMCS-OPD) from 2003 to 2011, and National Hospital Ambulatory Medical Care Survey Hospital Emergency Departments (NHAMCS-ED) from 2003 to 2014 were aggregated for this analysis. The number of prescriptions for isotretinoin and/or systemic corticosteroids was estimated by specialty (for NAMCS) and by survey type (for NHAMCS-OPD and NHAMCS-ED).
Results. Among all first visits to a physician for acne (n=18,914,096), approximately 3.9 percent prescribed isotretinoin, 0.24 percent prescribed corticosteroids, and the remaining 96 percent prescribed neither drug. This was comparable to estimates for first visits to a dermatologist for acne (n=13,920,913), where approximately 4.2 percent prescribed isotretinoin, 0.32 percent prescribed corticosteroids, and the remaining 95 percent prescribed neither medication.
Conclusion. Currently, isotretinoin and systemic corticosteroids are rarely prescribed together.
KEYWORDS: Acne, corticosteroids, isotretinoin
Acne is a common condition treated by dermatologists and other physicians.1,2 Severe acne often requires systemic therapy, such as isotretinoin.1 While isotretinoin is one of the most effective treatments for severely inflamed and nodulocystic acne, acne lesions can, paradoxically, flare or worsen with initiation of isotretinoin treatment.3 Prescribing isotretinoin at a low dose or concurrently prescribing systemic corticosteroids might help prevent these flares.1,4 If a flare in acne due to isotretinoin occurs, the concomitant use of systemic corticosteroids might help improve skin lesions and, although rare, might prevent systemic symptoms associated with acne fulminans.1,3
To our knowledge, there are no estimates in the literature on the frequency of coprescription of isotretinoin and systemic corticosteroids. Given the utility of systemic corticosteroids in decreasing acne flares, this study sought to quantify the estimated frequency of the coprescribing isotretinoin and systemic corticosteroids. We also aimed to assess trends in the use of isotretinoin with systemic corticosteroids for acne as they relate to age, sex, race, insurance, and provider specialty.
Methods
Data from the National Ambulatory Medical Care Survey (NAMCS) from 2003 to 2015, National Hospital Ambulatory Medical Care Survey Hospital Outpatient Departments (NHAMCS-OPD) from 2003 to 2011, and National Hospital Ambulatory Medical Care Survey Hospital Emergency Departments (NHAMCS-ED) from 2003 to 2014 were aggregated for this analysis.5–9 The number of prescriptions for isotretinoin and/or systemic corticosteroids was estimated by specialty (for NAMCS) and by survey type (for NHAMCS-OPD and NHAMCS-ED). Visits were stratified and weighted to reflect their clustered sampling probability as described by the National Center for Healthcare Statistics.10 A visit was considered as being “for acne” if the reason for the visit (or broad reason for the visit) listed “acne or pimples” or if the diagnosis listed “acne varioliformis” or “other acne.”
A multivariable logistic regression model for complex samples was used to estimate the odds of prescribing isotretinoin during a visit for acne as a function of survey year, age at time of visit, sex, race, insurance, and physician specialty. A similar approach was used to estimate the odds of prescribing a corticosteroid, though due to too few visits prescribing corticosteroids, survey year and insurance were not considered as covariates in the model. Regarding specialty, visits in the emergency department and outpatient department datasets were considered as being “nondermatology” visits.
Results
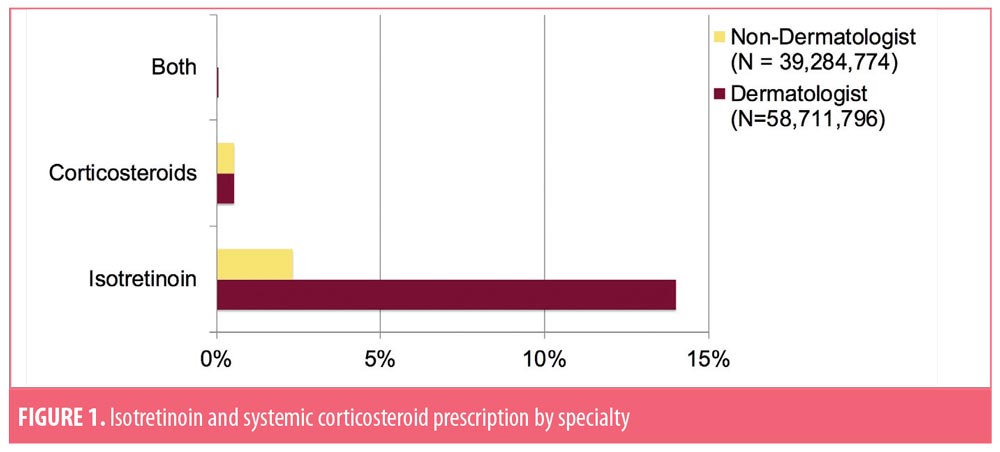
Between 2003 and 2015, a total of 97,996,570 visits for acne occurred. Among visits to dermatologists for acne (n=58,711,796), approximately 14 percent prescribed isotretinoin, 0.53 percent prescribed corticosteroids, and 0.04 percent prescribed both isotretinoin and corticosteroids (Figure 1). The remaining 85 percent prescribed neither. These estimates differed from visits to nondermatologists for acne (n=39,284,774), where 2.33 percent prescribed isotretinoin, 0.54 percent prescribed corticosteroids, and zero prescribed isotretinoin and corticosteroids. The remaining 97 percent mentioned neither drug.
For all first visits to a physician for acne, including dermatologists, (n=18,914,096), approximately 3.9 percent prescribed isotretinoin, 0.24 percent prescribed corticosteroids, and the remaining 96 percent mentioned neither drug. Among first visits to a dermatologist for acne (n=13,920,913), approximately 4.2 percent prescribed isotretinoin, 0.32 percent prescribed corticosteroids, and the remaining 95 percent mentioned neither medication. In this sample of data, age (p=0.24), race (p=0.39), sex (p=0.71), and physician specialty (p=0.90) were not associated with the use of a corticosteroid during a visit for acne (Table 1). Similarly, insurance was not associated with the use of isotretinoin.
Visits to dermatologists were 7.73 times more likely to prescribe isotretinoin than visits to nondermatologists (p<0.001) even after controlling for survey year, age, race, sex, and insurance (95% confidence interval [CI]: 4.38–13.66). Controlling for all other variables in the model, patients between the ages of 20 and 35 years were 1.93 times more likely to be prescribed isotretinoin compared with patients older than 35 years (95% CI: 1.27–2.91, p=0.002), as were patients younger than 20 years of age (OR: 2.75, 95% CI: 1.81–4.18; p<0.001). Controlling for all other variables in the model, those who identified as white were more likely than those who did not identify as white to receive a prescription for isotretinoin (OR: 1.65, 95% CI: 1.08–2.53; p=0.01), as were men (OR: 1.50, 95% CI: 1.10–2.04; p=0.01).
Limitations
The NAMCS does not include medication dosages, acne type, or acne severity, which limits inferences in prescribing patterns. Also, there might have been other disorders for which the corticosteroid was prescribed at these visits.
Conclusion
The coprescription of isotretinoin and systemic corticosteroids is very rare. These results suggest that either many physicians are not experiencing the paradoxical acne flare previously reported in the literature,1 are initiating low-dose isotretinoin to minimize the risk of a flare, are decreasing the dose of isotretinoin in response to a flare, or are unaware of the utility of the coprescription of systemic corticosteroids with isotretinoin. Dermatologists are more likely than other specialties to prescribe isotretinoin, which might be attributed to the greater severity of acne seen by dermatologists and the level of comfort of isotretinoin use developed during specialty training.
References
- Webster G. Acne vulgaris. BMJ. 2002;325(7362):475–479.
- Abokwidir M, Davis SA, Fleischer AB, Pichardo-Geisinger RO. Use of the emergency department for dermatologic care in the United States by ethnic group. J Dermatolog Treat. 2015;26(4): 392–394.
- Massa AF, Burmeister L, Bass D, et al. Acne fulminans: treatment experience from 26 patients. Dermatology. 2017;233(2–3):136–140.
- Borghi A, Mantovani L, Minghetti S, et al. Acute acne flare following isotretinoin administration: potential protective role of low starting dose. Dermatology. 2009;218(2):178–180.
- Ahn CS, Allen MM, Davis SA, et al. The National Ambulatory Medical Care Survey: a resource for understanding the outpatient dermatology treatment. J Dermatolog Treat. 2014;25(6): 453–458.
- Ahn CS, Davis SA, Dabade TS, et al. Noncosmetic skin-related procedures performed in the United States: an analysis of national ambulatory medical care survey data from 1995 to 2010. Dermatol Surg. 2013;39(12):1912–1921.
- Farhangian ME, Snyder A, Huang KE, et al. Cutaneous cryosurgery in the United States. J Dermatolog Treat. 2016;27(1):91–94.
- Koelblinger P, Dabade TS, Gustafson CJ, et al. Skin manifestations of outpatient adverse drug events in the United States: a national analysis. J Cutan Med Surg. 2013;17(4):269–275.
- Chen CL, Fitzpatrick L, Kamel H. Who uses the emergency department for dermatologic care? a statewide analysis. J Am Acad Dermatol. 2014;71(2):308–313.
- Hing E, Gousen S, Shimizu I, Burt C. Guide to using masked design variables to estimate standard errors in public use files of the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey. Inquiry. 2003/2004;40(4):416-415.