
Shannon M. Campbell, DO, Ohio University College of Osteopathic Medicine, Department of Specialty Medicine, O’Bleness Memorial Hospital, Athens, Ohio; Sara B. Peters, MD, The Ohio State University, Division of Dermatopathology, Columbus, Ohio; Matthew J. Zirwas, MD, The Ohio State University, Division of Dermatology, Columbus, Ohio; Henry K. Wong, MD, The Ohio State University, Division of Dermatology, Columbus, Ohio
Disclosure: Drs. Campbell, Peters, and Zirwas have no conflict of interests to declare. Dr. Wong has served as an advisor for EISAI.
Abstract
The application of CD markers to medicine has advanced our understanding of several dermatological diseases, most notably primary cutaneous lymphomas. CD markers are monoclonal antibodies that target cell surface molecules on leukocytes and antigens from other cells. T-cell processes are typically CD3+, CD20-, CD45+ while B-cell processes are typically CD3-, CD20+, and CD45+. Other CD markers are used to further delineate cutaneous lymphomas. Although an imperfect system, CD markers empower dermatologists to synthesize immunophenotyping with clinical findings and formulate an appropriate diagnosis. (J Clin Aesthet Dermatol. 2010;3(10):21–25.)
Advances in immunology have led to the categorization of numerous cellular subsets including T-cells, B-cells, and antigen-presenting cells that play a role in the immune response. With many cells having similar morphological features, the distinction of subsets has advanced with the identification of cell lineages using monoclonal antibodies targeted at surface proteins. The ability to detect cell types through the use of specific monoclonal antibodies directed at surface markers has valuable clinical and diagnostic implications.
Over time, immunophenotyping has become a powerful tool in classifying and organizing several types of diseases, from infectious to inflammatory to neoplastic. Cutaneous oncology has embraced the utilization of CD markers to help identify the origin and type of neoplastic processes, especially in regard to cutaneous T-cell and B-cell lymphomas. As more immunophenotypic markers become available and are incorporated into standard practice, it is essential that clinical dermatologists become familiar with interpreting the results to better serve patients and partner effectively with pathologists for accurate diagnosis. The objective of this article is to review the immunophenotyping in the pathological diagnosis of primary cutaneous lymphomas and give the dermatologist a greater understanding of how to apply this knowledge to everyday practice.
History and Role of CD Markers in Medicine
CD markers, an abbreviation for human cluster of differentiation markers, or cluster of designation (CD) markers, are a classification system for monoclonal antibodies against cell surface molecules on leukocytes and antigens from other cells.[1-3] The use of CD marker nomenclature was proposed in 1982 at the First International Workshop and Conference on Human Leukocyte Differentiation Antigens (HLDA), a conference now known as Human Cell Differentiation Molecules (HCDM). Many efforts continue to refine CD marker nomenclature and create a universal standard for laboratories across the world to apply when testing for CD markers.[2] CD markers must have at least two monoclonal antibodies for each antigen. A “w” indicates that the CD is not well characterized or is represented by only one monoclonal antibody. Currently, more than 400 CD markers have been identified, although not all of them are of diagnostic value.[2,3]
Immunophenotyping can be used on paraffin-embedded samples, frozen sections, or with flow cytometry. Some antibodies do not work with sections cut from paraffin-embedded samples or with frozen sections and necessitate flow cytometry. However, flow cytometry requires that cells being immunophenotyped be individually suspended in liquid, an easy task for circulating cells in peripheral blood samples, but more complicated when dealing with skin samples.[4]
Interpretation of CD marker staining on fixed tissue samples should be based on the cellular distribution of staining (i.e., membranous, cytoplasmic, nuclear), proportion of positively stained cells, and staining intensity. Cells are said to stain positive if a convincing appropriate pattern is visible and, conversely, stain negative if no or inconclusive staining is observed. The degree of positivity is graded subjectively by the dermatopathologist using adjectives, such as weak, moderate, or strong, to describe the intensity of staining and does not always directly correspond to the diagnostic significance of that particular stain. Negative and positive controls are also used in the staining process to allow for comparison, to confirm the specificity and sensitivity of the staining process, and to assist in determining the affinity of a particular stain.[3]
Although the utilization of CD markers has transformed our knowledge of cutaneous oncology, their use remains fraught with challenges. In theory, some CD markers are specific for a particular cell type or origin, but there can be overlap. Given that a single precursor cell can give rise to different kinds of mature cells, markers that indicate a common developmental lineage may be expressed and seen in different cell types. As a result, CD markers serve as an imperfect attempt to identify and classify some neoplastic cells. It is probably more accurate and practical to state that the pattern of CD marker expression is strongly suggestive of a certain cell type or lineage, but may not be definitive. In addition, the staining of CD markers is influenced by several factors, including tissue fixation and processing, which can affect their interpretation.[4,5] In the end, the use of multiple CD markers simultaneously yields the most accurate characterization of the neoplastic cell.
In this article, the authors offer a general approach to the pathological diagnosis of different types of cutaneous T-cell and B-cell lymphomas. For simplicity’s sake, the process of interpreting CD markers is presented in an algorithmic fashion, but this should not detract from the integration of several clinical and pathological factors required in making a diagnosis of primary cutaneous T-cell or B-cell lymphoma. Furthermore, it should be noted that although staining was presented in a stepwise manner, many laboratories and dermatopathologists use several stains concurrently to confirm or exclude a diagnosis.
Immunophenotyping in the Diagnosis of Primary Cutaneous Lymphomas
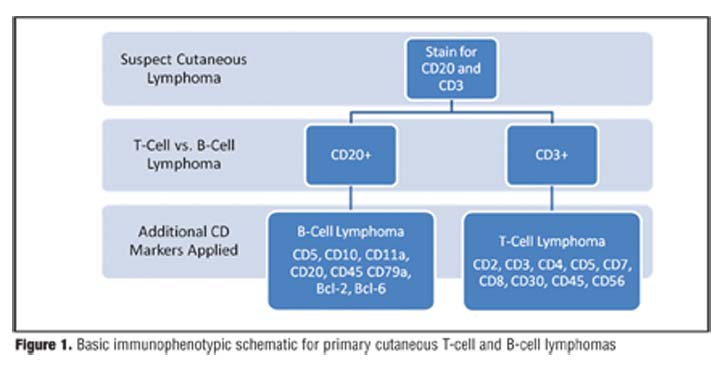
When faced with a possible cutaneous lympho-proliferative disorder, the dermatopathologist evaluates the overall histological architectural pattern of the biopsy while taking into account the clinical differential diagnosis supplied by the clinician. The first step in the immunophenotypic evaluation of these cases is determination if the dominant population of cells are B-cells, T-cells, or neither. Three markers are typically used for this initial classification: CD20, CD3, and CD45. CD20 is the most consistently positive marker for B-cells, CD3 is the most consistently positive marker for T-cells, and CD45 (also known as common leukocyte antigen or CLA) is a marker for bone marrow-derived leukocytes. T-cell processes are typically CD3+, CD20-, CD45+. B-cell processes are typically CD3-, CD20+, and CD45+. Processes in which the infiltrating leukocytes are neither T-cells or B-cells, such as some cases of leukemia cutis, are typically CD3-, CD20-, and CD45+.[6]
T-Cell Disorders
After recognizing that T-cells predominate, a host of other CD markers are used to characterize the cells further ( Figure 1 ). Commonly, staining for CD2, CD4, CD5, CD7, and CD8 is done. Expression of CD2 and CD3 confirms the presence of a T-cell process. The type of T-cells, whether CD4 and/or CD8, provides insight into the nature of the disease as an inflammatory or malignant process or combination thereof. The expression of CD5 and CD7 is variable depending on the disease process. The absence or reduced presence of CD7 can be suggestive of a diagnosis of cutaneous T-cell lymphoma (CTCL), as CD7 is frequently the first CD marker to lose expression in CTCL. However, it should be noted that loss of CD7 can occur in benign processes as well. Loss of other markers can also occur in CTCL. In erythroderma associated with Sezary syndrome, loss of CD26 is frequently seen.
{kind=link}
In addition to the qualitative evaluation of CD marker expression (positive, decreased, negative), a quantitative assessment is made regarding the CD4:CD8 ratio, which has a normal value of 2:1.7 An increased CD4:CD8 ratio is typically found in classic patch stage mycosis fungoides (MF)/CTCL, which decreases in more advanced stages of the disease. Nonetheless, there are unusual CTCL variants with a decreased CD4:CD8 ratio.6 In Sezary syndrome, the CD4:CD8 ratio is typically greater than 10.8 In addition to immunophenotyping, T-cell receptor gene rearrangement analysis can also assist in the diagnosis of CTCL.
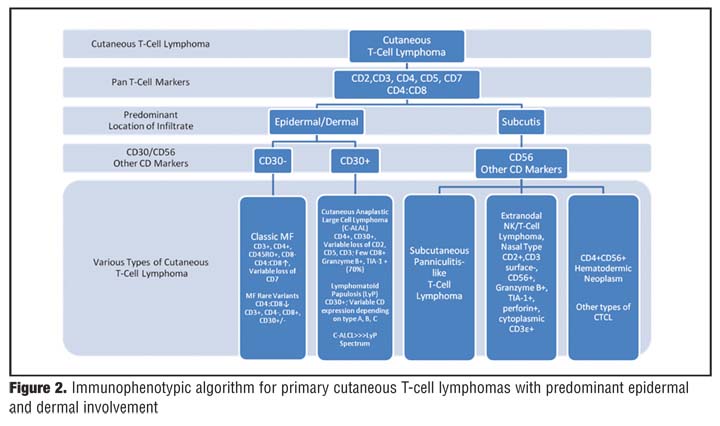
The location of the T-cell proliferation infiltrate can also influence how CD markers are used. If the T-cell proliferation localizes to the epidermis and/or dermis, staining for CD30 is traditionally used. This divides T-cell lymphomas into a CD30-negative group that includes classic mycosis fungoides and variants of CTCL that typically have an increased CD4:CD8 ratio and a CD30-positive group that includes cutaneous anaplastic large cell lymphoma (C-ALCL), lymphomatoid papulosis (LyP), and the C-ALCL-LyP spectrum (Figure 2).
{kind=link}
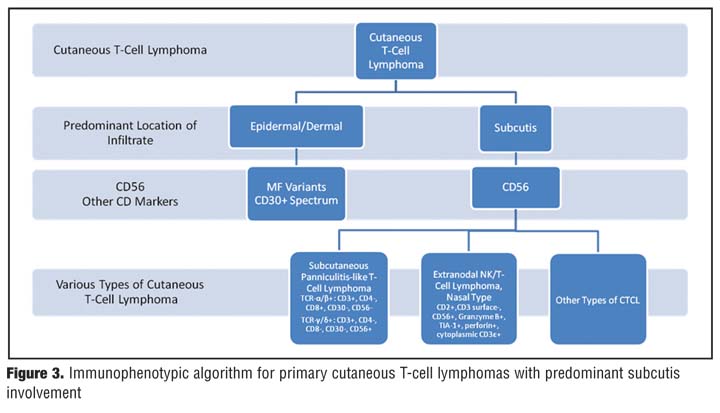
In contrast, if the T-cell infiltrate centers toward the lower dermis and into the subcutaneous tissue, the specimen may be stained for CD56 (Figure 3), a marker found on natural killer (NK) cells, a subset of T-cells, and often found to be positive in panniculitis-like T-cell lymphomas.6 Further testing to identify the tumor’s immunophenotype can then be used. In subcutaneous panniculitis-like-T-cell lymphoma (SPTL), there are two major T-cell phenotypic variants: a/b+ and g/d+. The majority of SPTL is of the g/d+ T-cell receptor (TCR) type, which is CD3+, CD4-, and CD8+ and rarely expresses CD56 and CD30. In contrast, the g/d phenotype is CD3+, CD4-, CD8- with common expression of CD56 and occasional expression of CD30. These phenotypical differences are important as the a/b+ type runs an indolent clinical course while the g/d+ type exhibits aggressive clinical behavior. Furthermore, in the World Health Organization-European Organization for Research and Treatment of Cancer (WHO-EORTC) classification system, only the g/d+ type is classified as a SPTL. The a/b+ variant is considered a type of cutaneous g/d+ T-cell lymphoma.9,10 Extranodal NK-T-cell lymphoma-nasal type usually expresses CD2, CD56, cytoplasmic CD3e and granzyme B, T-cell intracellular antigen-1 (TIA-1), and perforin and lacks surface CD3.[6,11]
{kind=link}
Immunohistochemistry in the Diagnosis of B-Cell Lymphomas
If the lymphocytic proliferation stains positive with CD20, a B-cell immunophenotypic work-up is warranted and includes CD5, CD10, CD43, CD79a, Bcl-2, and Bcl-6 ( Figure 1 ). CD5, CD20, and CD79a are pan B-cell markers. CD10 is a characteristic marker of follicular center cells and follicular lymphoma. Bcl-2 is an oncogene and positive in nodal follicular center cell lymphomas with chromosomal translocation.[12] Bcl-6 encodes a zinc finger transcriptional repressor that is needed for germinal center formation and has been implicated in the pathogenesis of some human lymphomas.[13] CD43 staining is applied to distinguish lymphoid hyperplasia from pulmonary mucosa associated lymphoid tissue (MALT) lymphoma.
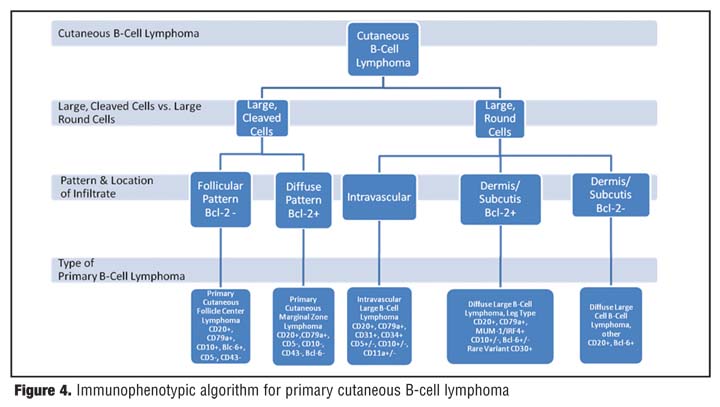
For cutaneous B-cell lymphomas, the predominant cell type is also identified based on morphological characteristics to aid in diagnosis (Figure 4). B-cells are described as either large, round cells or large, cleaved cells with the latter suggestive of primary cutaneous follicle center lymphoma (PCFCL) or primary cutaneous marginal zone lymphoma (PCMZL). PCFCL stains positive for CD20 and CD79a and shows a follicular pattern. CD10 is expressed in the follicular pattern and is typically negative in the diffuse pattern. Both follicular and diffuse patterns of PCFCL are typically Bcl-6 positive and Bcl-2, CD5, and CD43 are negative. If Bcl-2 stains positive, it should raise concern for a nodal etiology with skin trophism. PCMZL typically stains positively for CD20, CD79a, and Bcl-2 while staining for CD5, CD10, CD43, and Bcl-6 are negative.[14]
{kind=link}
If the predominant B-cell populations consist of large, round cells, then the location of those cells guides the next step in diagnosis (Figure 4). Large round cells located within blood vessels are diagnostic for cutaneous intravascular large B-cell lymphoma. Endothelial cell-related antibodies, such as CD31 or CD34, may be used to emphasize the intravascular location of those cells.
Intravascular large B-cell lymphoma expresses CD20 and CD79a and may atypically express CD5, CD10, and CD11a.[6,14] CD11a mediates leukocyte adhesion to endothelium, leukocyte trafficking through activated endothelium, and lymphocyte blastogenesis.[3]
Conversely, if the large, round cells reside in the dermis and/or subcutis, staining for Bcl-2 helps to refine the diagnosis. Positive staining of Bcl-2 is suggestive of diffuse large B-cell lymphoma, leg type (DLBCLLT) and negative staining is indicative of diffuse large B-cell lymphoma, other. DLBCLLT demonstrates positivity for CD20, CD79a, and Bcl-2 in the majority of cases and commonly express Bcl-6 and/or CD10. In addition, DLBCLLT stains positive for MUM-1/IRF4 (multiple myeloma oncogene 1 or interferon regulatory factor 4), a marker for germinal center plasma cells, which helps to differentiate it from the diffuse form of follicle center lymphoma. In addition, there is a rare variant of DLBCLLT that stains positive for CD30.[14]
Diffuse large cell B-cell lymphoma, other (DLCBCL) demonstrates a diffuse growth pattern of large round transformed B-cells that do not share the characteristics of DLBCLLT or T-cells and is usually Bcl-2 negative. Typically, DLCBCL is Bcl-6 positive and expresses other common B-cell markers. It may be positive or negative for Bcl-2.[6,14,15]
Primary versus Secondary Cutaneous Lymphomas
In contrast to primary cutaneous lymphomas, secondary cutaneous lymphomas show a B-cell predominance. A patient diagnosed with cutaneous B-cell lymphoma must undergo a complete systemic work-up with a thorough review of systems, physical examination, and studies that include computed tomography scans and bone marrow biopsy, to determine if the B-cell lymphoma is primary or if it is a systemic B-cell lymphoma involving the skin secondarily. T-cell lymphomas involving the skin, while also capable of arising extracutaneously or spreading to extracutaneous sites, are more frequently skin limited and appropriate staging is important for directing therapy. Further work-up for these patients is directed based on findings from a thorough physical exam, including lymph nodes, and review of systems.
Conclusion
Immunophenotyping of cutaneous lymphoma has become standard practice for accurate diagnosis. The clinical dermatologist requires a general understanding of how immunophenotyping is used to characterize a lymphocytic proliferation when reviewing a pathology report and correlating it with clinical findings. While the practice of immunohistochemistry is fallible, a better appreciation of its role in the diagnosis of primary cutaneous lymphomas will enable the practicing dermatologist to collaborate more successfully with the dermatopathologist, leading to more rapid and accurate diagnosis of patients presenting within this spectrum of disease.
References
1. Ellmark P, Woolfson A, Belov L, Christopherson RI. The applicability of a cluster of differentiation monoclonal antibody microarray to the diagnosis of human disease. Methods Mol Biol. 2008;439:199–209.
2. Heddy Z, Swart B, Nicholson I, et al. CD molecules 2005: human cell differentiation molecules. Blood. 2005;106(9): 3123–3126.
3. Zola H, Swart B, Nicholson I, Voss E, eds. Leukocyte and Stromal Cell Molecules: The CD Markers. Hoboken, New Jersey: John Wiley and Sons; 2007.
4. Fritschy JM. Is my antibody-staining specific? How to deal with pitfalls of immunohistochemistry. Eur J Neurosci. 2008;28(12):2365–2370.
5. MacIntyre N. Unmasking antigens for immunohistochemistry. Br J Biomed Sci. 2001;58(3):190–196.
6. Strutton, Jeffrey. Cutaneous infiltrates: lymphomatous and leukemic. In: Weedon D, ed. Skin Pathology. 3rd ed. Philadelphia, Pa: Churchhill Livingston; 2010:971–1005.
7. McPherson RA. Overview of the immune system and immunologic disorders. In: McPherson RA, Pincus MR. Henry’s Clinical Diagnosis and Management by Laboratory Methods. 20th ed. Philadelphia, Pa: WB Saunders Co; 2001:817–820.
8. Vonderheid EC, Bernengo MG, Burg G, et al. An update on erythrodermic cutaneous T-cell lymphoma: report of the International Society for Cutaneous Lymphomas. J Am Acad Dermatol. 2002;46(1):95–106.
9. Willemze R, Kerl H, Sterry W, et al. EORTC classification for primary cutaneous lymphomas: a proposal from the Cutaneous Lymphoma Study Group of the European Organization for Research and Treatment of Cancer. Blood. 1997;90(1):354–371.
10. Jaffe ES, Harris NL, Stein H, Vardiman JW, eds. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of Haematopoeitic and Lymphoid Tissues. Lyon, France: IARC Press; 2001.
11. Willemze R. Cutaneous T-cell lymphoma. In: Bolognia JL, Jorrizzo JL, Rapini RP, editors. Dermatology. 2nd ed. Spain: Elsevier; 2008 p. 1867-86.
12. Miyashita T, Reed JC. Bcl-2 oncoprotein blocks chemotherapy-induced apoptosis in a human leukemia cell line. Blood. 1993;81:151–157.
13. Baron BW, Nucifora G, McCabe N, et al. Identification of the gene associated with the recurring chromosomal translocations t(3;14)(q27;q32) and t(3;22)(q27;q11) in B-cell lymphomas. Proc Natl Acad Sci USA. 1993;90(11):5262–5266.
14. Cerroni L. B-cell lymphomas of the skin. In: Bolognia JL, Jorrizzo JL, Rapini RP, editors. Dermatology. 2nd ed. Spain: Elsevier; 2008 p. 1855-65.
15. Kodama K, Massone C, Chott A, et al. Primary cutaneous large B-cell lymphomas: clinicopathologic features, classification, and prognostic factors in a large series of patients. Blood. 2005;106(7):2491–2497.