
Uwe Wollina, MD; Yousef Bayyoud, MD; Thomas Kittner, MD; Eberhard Dürig, MD
Uwe Wollina, MD is from Department of Dermatology and Allergology; Yousef Bayyoud, MD is from Neurosurgical Unit, Department of Emergency and Reconstructive Surgery; Thomas Kittner, MD is from Department of Radiology; Eberhard Dürig, MD is from Institute of Pathology, “Georg Schmorl,” Academic Teaching Hospital Dresden-Friedrichstadt, Dresden, Germany
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Tricholemmal squamous cell carcinoma is a rare variant of squamous cell carcinoma thought to follow a more benign course. The authors present the case of a 67-year-old man with a giant tricholemmal squamous cell carcinoma on his scalp. Further investigations demonstrated a skull destruction and cranial invasion. Curative treatment was impossible, but tumor mass reduction and wound closure by sandwich split-thickness skin mesh graft transplantation using a dermal template was performed. Problems of advanced squamous cell carcinoma on the scalp are discussed.
(J Clin Aesthet Dermatol. 2011;4(4):34–37.)
Squamous cell carcinoma (SSC) of the skin is a common cancer among Caucasians in their second half of life. The most common affected body part is the head and neck region. According to data from the Cancer Registry of the Federal State of Saarland, Germany, during 1995 to 1999, age-standardized incidence rates were 11.2 per 100,000 for men and 4.4 per 100,000 for women.[1]
SSC prognosis is dependent on tumor size and location, differentiation, and the histological subtype. In a multivariate analysis of 615 patients with SCC, key prognostic factors for metastasis were increased tumor thickness (>2mm), immunosuppression, localization on the ear, and increased diameter (>6mm). The risk of local recurrence was increased in thicker tumors and SCC with desmoplasia.2 High-risk SCC are also seen on genital skin, lips, and after recurrence.
Focal tricholemmal differentiation is seen in SCC with clear cells, but tricholemmal SCC is quite rare.[3] Tricholemmal SCC is most often seen in the head and neck region and is generally thought to run a more benign course.[4–6]
This tumor type is characterized by abundance of glycogen-rich, clear cells with foci of pilar-type keratin-ization, peripheral palisading of cells, and subnuclear vacuolization.[6] High mitotic rate seems to be a constant feature.[7] This tumor type has also been called tricholemmal or trichilemmal carcinoma.[6]
The authors report a case of a giant tricholemmal SCC with cranial invasion.
Case report
A tall, 67-year-old, homeless man presented to the emergency room with a bleeding, ulcerated, malodorous, exophytic, giant tumor of the scalp, which was infested with maggots (height 170cm; weight 52kg). An alcoholic who neglected his health, he presented with mild edema of the lower legs and generalized xerotic skin. No other pathologies were detected. His medical history and the family history were unremarkable. He had no medical drug therapy.
Two years earlier, the patient had presented after a minor traffic accident for the suturing of soft tissue wounds. Documented in his file from this incident was a 2x3cm exophytic skin tumor in the same scalp area as the present tumor. Tumor excision had been recommended, but the patient refused to have surgery for tumor removal. He was lost for follow up.
Clinical findings. After mechanical removal of maggots, the tumor presented with a cauliflower-like exophytic growth with partial superficial necrosis and discharge (Figure 1). The tumor was 23cm x 12cm x 2.4cm (as measured by computerized tomography [CT]) and was localized in the midline of the frontal skull. There were neither clinical signs of tumor spread to regional lymph nodes nor any neurological impairment.
{kind=link}
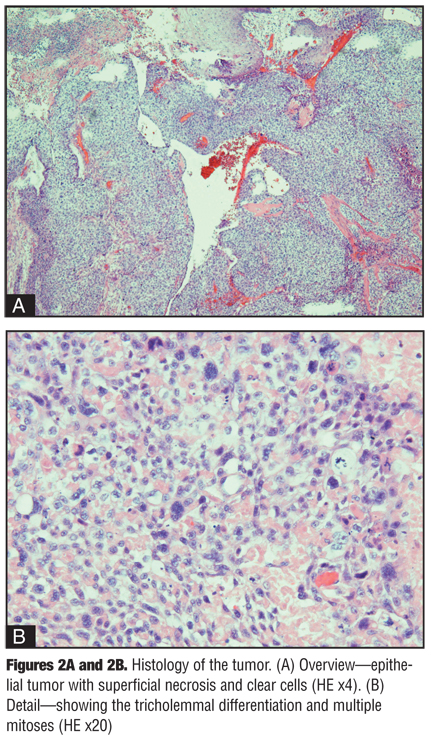
A diagnostic biopsy was taken. The histology described squamous epithelial strands and proliferations with only occasional connections to the overlying epidermis. There was cellular and nuclear polymorphism with numerous, partly atypical mitoses. In larger parts of the tumor, clear cells were the dominant cell type with a tricholemmal differentiation. In the outer parts of the tumor, some palisading of tumor cells was seen. The whole tumor showed a low level of differentiation according to Broders grade 3 (Figure 2). The diagnosis of a tricholemmal SCC was made.
Routine laboratory exam demonstrated anemia and hypoproteinemia: erythrocyte count 3.1Tpt/L (normal range 4.6–6.2), hemoglobin 6.4mmol/L (normal range 8.6–12.1), and serum protein 43.3g/L (normal range 60–85). Microbial swabs from the tumor surface revealed Proteus mirabilis, Alcaligens faecalis, and beta-hemolysing streptococci that were sensitive to levofloxacin.
{kind=link}
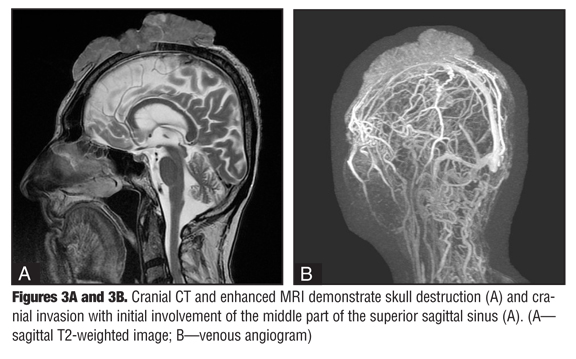
Staging with thoracic X-ray, lymph node sonography, and cranial computerized tomography (CCT) did not show any metastasis. Cranial CT, magnetic resonance imaging (MRI), and gadolinium-enhanced vascular MRI disclosed parietal parasagittal cranial tumor invasion. There was a continuous growth to the meninges on the left side with infiltration (3.5 x 3.7cm) and partial closure of the medial part of the superior sinus sagittalis (remaining open lumen 2.4cm) (Figure 3).
{kind=link}
Treatment and course. The authors cleaned and disinfected the tumor-induced ulcerations and initiated intravenous antibiotic therapy (levofloxacin 250mg twice daily). Under general anesthesia, tumor debulking surgery was performed with clinical safety margins ?2cm laterally down to the skull. During surgery, a blood transfusion was performed to normalize anemia and improve wound healing.
In the central part of the tumor, a large skull defect due to tumor invasion was visible. Because of the neighboring superior sagittal sinus, the authors decided to perform an incomplete resection since the risk of major bleeding and brain edema was evident. The tumor was removed to the level of the skull bone (R2 resection). The defect was covered by oxygenized regenerated cellulosis (Tabotamp, Johnson & Johnson—Ethicon) and split-thickness skin mesh graft transplant.
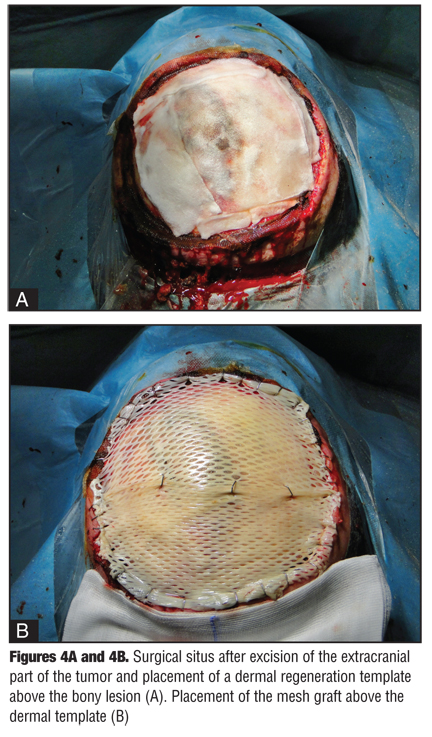
There was an uneventful postoperative course and the patient could leave the intensive care unit after 24 hours, but the transplant was avital after seven days. The authors performed a second surgery with complete debridement of the defect and thinning of the outer tabula of the skull bone by a larger rose drill. After that, a smaller rose drill was used to make penetrations into the spongiosa to reach diploe veins for transplant nutrition. The whole area was covered with a dermal template of porcine collagen (mediCipio, V-CARE Biomedical Leipzig). Split skin was obtained from the abdomen, meshed 1:1.5, and transplanted onto the dermal template (Figure 4). A light protective helmet was provided to support mobilization (Figure 5). The patient was referred to the radio-onocology unit for palliative radio-therapy after transplant healing.
{kind=link}
{kind=link}
Discussion
This case is remarkable in several ways. The patient presented with a giant scalp tumor that was diag-nosed as tricholemmal SCC. His subtype of SCC is thought to have a favorable prognosis.[4–6] Considering key prognostic factors of SCC, this patient had a high risk of metastasis due to tumor size and thickness.[2] In the present patient, however, the authors observed no metastatic spread, but a major cranial invasion.
Skull destruction and cranial invasion are uncommon features of cutaneous epithelial cancer.[8] Sundaram et al observed a delay of several years between SCC removal and cranial polyneuropathy due to perineural invasion.[9] In larger case series, perineural invasion has been observed in up to six percent of SCC cases.[10,11]
Cranial invasion, however, is rare.[12] Organ transplant recipients with alopecia, HIV-infected patients, and patients with scleroderma or burn scars of the scalp are at risk.[13–16] Cranial invasion is an independent negative prognostic factor.[17] In the present case, neglect by the patient led to the unfavorable tumor development.
Although Mohs surgery and its modifications represent the gold standard of treatment, in the present case an R0 resection would have only been possible with ligation of the middle part of the superior sinus sagittalis. That bears a major risk of brain edema and has a high mortality. Comparable cases have been reported from Japan by Sakamoto et al.[18] Therefore, the authors decided to follow a different course. After extensive debulking tumor surgery of the scalp down to the bone, a dermal regeneration template was used for reconstruction of a large, full-thickness scalp defect.[19–22] After this, curative radiotherapy was planned followed by reconstruction of the destructed bony structures. Radiotherapy of cutaneous head and neck SCC is a widely accepted choice of treatment.[23–25] Curative radiotherapy before would have impeded closure of this large scalp defect.
In conclusion, this is the first report on aggressive tricholemmal SCC with cranial invasion. Because of the advanced stage of the disease, a curative treatment was impossible. Tricholemmal SCC should be removed by Mohs surgery in an early stage whenever possible.
References
1. Stang A, Stegmaier C, Jöckel KH. Nonmelanoma skin cancer in the Federal State of Saarland, Germany, 1995–1999. Br J Cancer. 2003;89(7):1205–1208.
2. Brantsch KD, Meisner C, Schönfisch B, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol. 2008;9(8):713–720.
3. Dalton SR, LeBoit PE. Squamous cell carcinoma with clear cells: how often is there evidence of tricholemmal differentiation? Am J Dermatopathol. 2008;30(4):333–339.
4. Cassarino DS, Derienzo DP, Barr RJ. Cutaneous squamous cell carcinoma: a comprehensive clinicopathologic classification—part two. J Cutan Pathol. 2006;33(4): 261–279.
5. Petter G, Haustein UF. Histologic subtyping and malignancy assessment of cutaneous squamous cell carcinoma. Dermatol Surg. 2000;26(6):521–530.
6. Wong TY, Suster S. Tricholemmal carcinoma. A clinicopathologic study of 13 cases. Am J Dermatopathol. 1994;16(5):463–473.
7. Boscaino A, Terracciano LM, Donofrio V, et al. Tricholemmal carcinoma: a study of seven cases. J Cutan Pathol. 1992;19(2):94–99.
8. Sedira MA, Amin AA, Rifaat MA, et al. Locally advanced tumors of the scalp: the Egyptian National Cancer Institute experience. J Egypt Nat Cancer Inst. 2006;18(3):250–257.
9. Sundaram AN, Simmons Z, Towfighi J, et al. Contralateral cranial polyneuropathy due to perineural invasion by a cutaneous squamous cell carcinoma. J Clin Neuromuscul Dis. 2010;11(3):132–136.
10. Cernea CR, Ferraz AR, de Castro IV, et al. Perineural invasion in aggressive skin carcinomas of the head and neck. Potentially dangerous but frequently overlooked. ORL J Otorhinolaryngol Relat Spec. 2009;71(1):21–26.
11. Mendenhall WM, Amdur RJ, Hinerman RW, et al. Skin cancer of the head and neck with perineural invasion. Am J Clin Oncol. 2007;30(1):93–96.
12. Etlik O, Bay A, Izmirli M, et al. Deep intracranial extension of squamous cell carcinoma of the scalp. Pediatr Blood Cancer. 2005;45(7):994–996.
13. Neubauer KE, Goldstein GD, Plumb SJ. Squamous cell carcinoma of the scalp in organ transplant recipients: exploring mechanisms for recurrence and treatment guidelines. Dermatol Surg. 2010;36(2):185–193.
14. Neves-Motta R, Ferry FR, Basílio-de-Oliveira CA, et al. Highly aggressive squamous cell carcinoma in an HIV-infected patients. Rev Soc Bras Med Trop. 2004;37(4):496–498.
15. Wollina U, Buslau M, Petrov I, Pramatarov K. Disabling pansclerotic morphea of childhood. Expert Review Dermatol. 2007;2(6):775–784.
16. Sakamoto T, Mineura K, Kikuchi K, et al. Surgical management of squamous-cell carcinomas arising in burn scar of the scalp [Japanese]. No Shinkei Geka. 1989;17(2):147–151.
17. Maghami EG, Talbot SG, Patel SG, et al. Craniofacial surgery for nonmelanoma skin malignancy: report of an international collaborative study. Head Neck. 2007;29(12):1136–1143.
18. Sakamoto T, Mineura K, Kikuchi K, Kowada M. Intracranial invasion of scalp carcinoma. Report of five cases. Acta Neurochir (Wien). 1989;98(1-2):66–69.
19. Abbas Khan MA, Chipp E, Hardwicke J, et al. The use of dermal regeneration template (Integra®) for reconstruction of a large full-thickness scalp and calvarial defect with exposed dura. J Plast Reconstr Aesthet Surg. 2010; in press.
20. Kinsella CR Jr, Grunwaldt LJ, Cooper GM, et al. Scalp reconstruction: regeneration with acellular dermal matrix. J Craniofac Surg. 2010;21(2):605–607.
21. Khan MA, Ali SN, Farid M, et al. Use of dermal regeneration template (Integra) for reconstruction of full-thickness complex oncologic scalp defects. J Craniofac Surg. 2010;21(3):905–909.
22. Faulhaber J, Felcht M, Teerling G, et al. Long-term results after reconstruction of full-thickness scalp defects with a dermal regeneration template. J Eur Acad Dermatol Venereol. 2010;24(5):572–577.
23. Garcia-Serra A, Hinerman RW, Mendenhall WM, et al. Carcinoma of the skin with perineural invasion. Head Neck. 2003;25(12):1027–1033.
24. Gluck I, Ibrahim M, Popovtzer A, et al. Skin cancer of the head and neck with perineural invasion: defining the clinical target volumes based on the pattern of failure. Int J Radiat Oncol Biol Phys. 2009;74(1):38–46.
25. Piccinno R, Caccialanza M. Radiotherapy of squamous cell carcinoma of the skin: indications and warnings. J Clin Dermatol. 2010;1(1):59–63.