
 by Hamzah Mustak, FCOphth (SA); Danica Fiaschetti, LVN, COA; Adit Gupta, MD; and Robert Goldberg, MD
by Hamzah Mustak, FCOphth (SA); Danica Fiaschetti, LVN, COA; Adit Gupta, MD; and Robert Goldberg, MD
Dr. Mustak is with the University of Cape Town Groote Schuur Hospital in Cape Town, Western Cape, South Africa. Drs. Mustak, Fiaschetti, Gupta, and Goldberg are with the Stein Eye Institute, University of California in Los Angeles, California.
Funding: No funding was provided for this article.
Disclosures: The authors have no conflicts of interest to relevant to the content of this article.
Abstract: Background. The eyebrow region presents challenges for filling: the skin is thick, the three-dimensional anatomy is complex and there is a predisposition towards fat atrophy and skeletonization with aging. Hyaluronic acid gel fillers are well known for their use in the periorbital region. We report our long-term experience with eyebrow filling over a period of five years.
Methods. Twenty cases of periorbital eyebrow filling with hyaluronic acid gel fillers were followed up over a period of five years. The eyebrow filling was customized based on the patient’s anatomical features in a three-dimensional plane. Standardized photographs before and after the procedure in standard lighting conditions were evaluated.
Results. Hyaluronic acid gel fillers were tolerated well in the eyebrow region. There were no cases with blue-gray dyschromia or prolonged edema as is the case with lower eyelid injections. The eyebrow gained volume and looked fuller immediately after the injection. There were three cases with excessive eyebrow puffiness noted on a long-term follow-up which may be the accumulated filler weighing the eyebrow. No other adverse events were noted.
Conclusion. The eyebrow anatomy is a complex three-dimensional structure. Deflation in the eyebrow area along with the superior sulcus occurs with aging. Filling the eyebrow with hyaluronic acid gel fillers is a useful tool in the armamentarium of the cosmetic facial surgeon and can be used in isolation in select patients or as an adjunct to surgical rehabilitation. We believe the fillers last longer and are well tolerated in the eyebrow region due to the complex anatomy specific to this region.
Keywords: Eyebrow, filler, facial rejuvenation
J Clin Aesthet Dermatol. 2018;11(2):38–40
Introduction
The eyelid-eyebrow unit plays an important role in facial aesthetics. The eyebrow is distinctive in its structure and forms the framework for the upper eyelid. In younger individuals, the eye looks longer and fuller with thicker, elastic skin. As we age, the skin loses elasticity, the tissues deflate, and the underlying bony orbital rim is exposed.1,2 In addition, the eyebrows simultaneously undergo characteristic aging changes. The brow position droops by a few millimeters, more laterally than medially, and the eyebrow fat pad shrinks, leading to a flatter appearance and loss of three-dimensional projection.1–3
Facial re-inflation has been practiced for centuries, with reports of paraffin being used in Greece in the early 19th century.4 Autologous fat injection, in combination with blepharoplasty and fillers, has been used with variable success in the peri-orbital region.5–7 Volume enhancement of the aging face, although not a substitute for conventional surgery, is a promising alternative.6,7,8 The concept of nonsurgical rejuvenation and tissue inflation rather than excision is gaining attention as our understanding of aging improves. There is a subset of patients who are poor candidates for surgical rejuvenation. For these patients, volume enhancement with hyaluronic acid gels is a promising treatment modality. When assessing the eyebrow unit aesthetically, it is important to differentiate the eyebrow hairs from the three-dimensional eyebrow shape. The geographic distribution of the eyebrow hairs can be altered by reduction (e.g., waxing, plucking, threading) or by augmentation (e.g., makeup, tattooing, microblading). The three-dimensional shape is very important in facial aesthetics and changes with aging; it can be improved with reduction (e.g., eyebrow fat debulking, orbital rim shaving) or augmentation (e.g., fat, synthetic fillers). In this retrospective chart review, we report our long-term experience with hyaluronic acid gels (HAG) as a treatment modality for adding volume to the three-dimensional eyebrow shape.
Methods
This retrospective study reviewed the charts of patients who were administered HAG. All the patients who had eyebrow filler injections within the past ten years with the following criteria were included: 1) minimum follow-up of five years; 2) no history of eyelid or eyebrow surgery within the follow-up duration; and 3) no history of neurological disease.
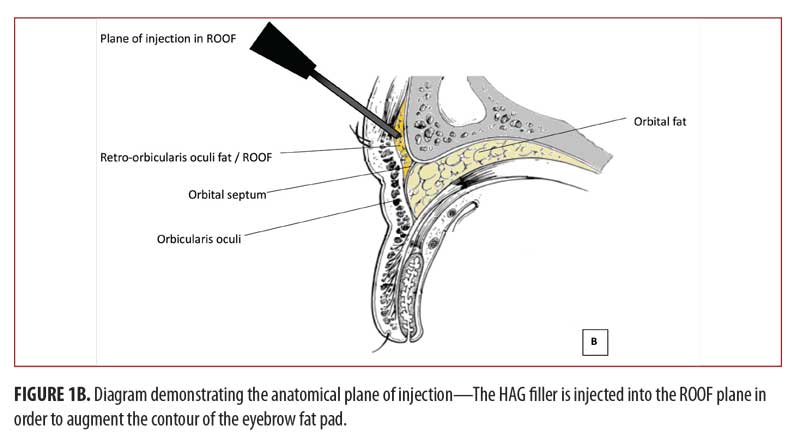
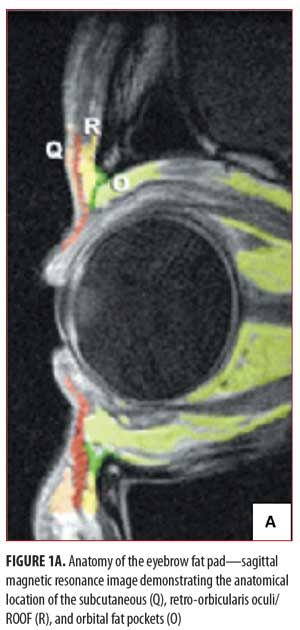
All the injections were performed by a single oculoplastic surgeon. Using the HAG Restylane-L (Galderma, Fort Worth, Texas), use of which was based on surgeon experience and preference. Injections were carried out under topical anesthesia that was applied 30 to 60 minutes before the procedure. Treatment area was sterilized with alcohol immediately before the injections. Using a 30-gauge needle, the HAG was applied in the retro-orbicularis oculi fat (ROOF) pad in the tissue plane deep to the orbicularis oculi muscle (Figure 1A–B). A feathering technique was employed using multiple passes of the needle to create a haystack configuration of multiple fine threads, layered and feathered to create the desired three-dimensional contour. Bruising is primarily associated with passage of the needle through the orbicularis layer. To minimize bruising, the needle is only withdrawn all the way out through the skin when repositioning is required or for another series of passages. Once the needle is deep to the orbicularis, the surgeon takes advantage of the sub-orbicularis plane by creating a fan-shaped pattern of passes without withdrawing the needle completely. If bruising or hematomas start to form, the area is treated with gentle pressure from a cotton tip applicator. If the needle is placed too superficially, visible lumps or wheals of the HAG will form. It is important, therefore, to avoid depositing large volumes of the filler in one location. Gentle, continuous pressure is applied to the syringe plunger as the needle is slowly fanned through the tissues to create smooth, feathered, three-dimensional contours. The shape is customized to the patient and the degree of volume, whether applied in the superior aspect of the eyebrow fat pad, the inferior aspect of the eyebrow fat pad, feathered laterally into the temporalis muscle fossa, or added along the deep orbital rim to fill the superior sulcus, will vary from patient to patient. A clinical effect with an appreciable change in eyebrow contour is visible during and immediately after the procedure.
Results
We collected data and analyzed photographs of 20 patients who had been followed for at least five years. There were three men and 17 women. Mean age was 53.5 years (32–62). Average amount of HAG injected was 4.3cc (3.2–8.6cc) over the five-year follow up period. Through example cases, we endeavor to demonstrate the importance of individualized analysis and customized filling.
Case 1 (Figure 2). Customization of the three-dimensional shape of the eyebrow. Figure 2A shows pretreatment view of a 64-year-old woman who presented with deflation of the lateral eyebrow fat. Figure 2B shows the injection pattern of 0.3cc HAG injected to both sides using a feathering technique to layer the product in a haystack fashion. The blue markings indicate the injection pattern utilized to create a layered three-dimensional contour. Figure 2C shows post-treatment view, displaying a fuller eyebrow with lifting of the lateral tail, resulting in a more youthful appearance.

Case 2 (Figure 3). Eyebrow projection. Figure 3A show the pretreatment view of the left side of a 46-year-old woman’s brow with deflation of the lateral eyebrow fat and drooping of the eyebrow tail. HAG 0.2cc was injected in the ROOF plane in order to augment the lateral brow volume. Figure 3B displays post-treatment results, showing a fuller eyebrow contour with enhanced projection of the lateral eyebrow.

Case 3 (Figure 4). Enhancement of the inferior eyebrow (ROOF) fat pad. Figures 4A and 4B show pretreatment view of a 50-year old woman with a hollow superior sulcus and deflation of the eyebrow with unveiling of the superior orbital rim (skeletonization). HAG 0.5cc was injected into the left eyebrow fat pad and 0.4cc into the right side in order to augment the sulcus hollowing as well as project the lateral eyebrow. Figures 4C and 4D show post-treatment frontal view (C) and lateral view (D) after HAG injection, demonstrating a softer, more youthful, three-dimensional contour of the superior sulcus-eyebrow complex.

There were no complications from the injections. None of the patients developed blue-grey dyschromia.9 The mean interval between repeat filler injection was 14 months (12–24). Over the follow-up period, we observed heavy eyebrows and puffiness in three patients.
Discussion
The upper orbital space is a key three-dimensional contour defining periorbital aesthetics.10 In youth, fullness of the dermis, subcutaneous fat pads, and deep fat pads create a three-dimensional fullness that defines the aesthetics of the youthful eyelid.1–3 With aging, loss of volume in the dermis and various fat pads can create a sagging appearance, drawing inelastic skin into the eyelid space and creating the appearance of eyebrow drooping.11 In addition, there is likely some actual gravitational descent of the lateral eyebrow, but this is generally less important than deflation in creating the aged appearance.
Rehabilitation of the aging upper orbit is most effective when this loss of volume is taken into account. Conversely, rehabilitative paradigms that focus primarily on elevating the eyebrow are suboptimal in re-creating the contours of youth. The smooth, full, three-dimensional shape created by the subcutaneous and deep fat pads characterizes the eyebrow.12,13 This contour covers the orbital rim and extends variably into the eyelid space itself. By projecting the skin forward, the three dimensional volume essentially elevates the eyelid skin out of the orbital space in a similar way that a full balloon stretches and smoothes the rubber surface. We noted heavy eyebrows and puffiness in three patients; this could have been due to the filler substance accumulation over repeated injections.
There have been various recommendations about the position of injection. Lucarelli and colleagues14 demonstrated that injecting in the pre-periosteal plane requires less volume while achieving a robust result. Lambros15 recommends injecting into the sub-orbicularis and subcutaneous fat, while Glasgold16 recommends injecting into the subcutaneous plane. The ROOF extends from the eyebrow region that drapes over the superior orbital rim to the upper eyelid. This fat pad contributes to the smooth contour over the superior orbital rim. We find that injecting into the plane of the ROOF is effective in creating smooth, appropriate contours. Growing out of this three-dimensional structure of the eyebrow fat pad and three-dimensional shape are the eyebrow hairs. The thickness, geographic distribution, and shape of the eyebrow hair vary substantially. Certainly, the eyebrow hairs effect appearance and are the subject of a vast industry focused on shaping, coloring, thinning, removing or tattooing hairs to effect the geographic distribution. We suggest avoiding being distracted by the distribution of the eyebrow hairs when assessing the three-dimensional shape of the eyebrow.
Conclusion
We have had good success filling the eyebrow fat pad to change the three-dimensional shape of the eyebrow complex. The shape of the eyebrow fat pad, and its extensions into the superior orbital space and temporalis fossa, varies across individuals. HAG filler alone is particularly useful for patients who are poor candidates for surgery or want to avoid surgery. It might also be a useful tool in conjunction with surgery to address the volume depletion seen with aging.
The primary goal of eyebrow surgery or filling should be to improve the three-dimensional shape of the eyebrow complex, rather than focusing on the distribution of the eyebrow hairs. For optimal results, the distribution of filler should be customized to the patient in an artistic manner. In our anecdotal experience, subtle sculpting of the shape of the eyebrow complex with HAG fillers can help achieve acceptable cosmetic endpoints for eyebrow contouring.
References
- Lambros V. Observations on periorbital and midface aging. Plast Reconstr Surg. 2007;120:1367–1376.
- Lambros V. Models of facial aging and implications for treatment. Clin Plast Surg. 2008;35:319–327.
- Shaw RB Jr, Katzel EB, Koltz PF, et al. Aging of the facial skeleton: aesthetic implications and rejuvenation strategies. Plast Reconstr Surg. 2011;127:374–383.
- Goldwyn RM. The paraffin story. Plast Reconstr Surg. 1980;65:517–522.
- Lambros V. Fat injection for the aging midface. Oper Tech Plast Reconstr Surg. 1998;5:130–137.
- Goldberg RA, Fiaschetti D. Filling the periorbital hollows with hyaluronic acid gel: initial experience with 244 injections. Ophthal Plast Reconstr Surg. 2006;22:335–341.
- Hoenig J, Hoenig D. Minimally invasive periorbital rejuvenation. Facial Plast Surg. 2013 Aug;29(4): 295–309.
- Kornstein AN. Soft-tissue reconstruction of the brow with Restylane. Plast Reconstr Surg. 2005;116: 2017–2020.
- Rootman DB, Lin JL, Goldberg R. Does the Tyndall effect describe the blue hue periodically observed in subdermal hyaluronic acid gel placement? Ophthal Plast Reconstr Surg. 2014;30:524–527
- Gunter JP, Antrobus SD. Aesthetic analysis of the eyebrows. Plast Reconstr Surg.1997;99(7):1808–1816.
- Papageorgiou KI, Mancini R, Garneau HC, et al. A three-dimensional construct of the aging eyebrow: the illusion of volume loss. Aesthet Surg J. 2012;32:46–57.
- Hwang SH, Hwang K, Jin S, et al. Location and nature of retro-orbicularis 141 oculus fat and suborbicularis oculi fat. J Craniofac Surg. 2007;18:387–390.
- Charpy M. Le coussinex adipoeux du sourcil. Bibliog Anat. 1909;19:47–52.
- Griepentrog GJ, Lucarelli MJ. Anatomical position of hyaluronic acid gel following injection to the eyebrow. Ophthal Plast Reconstr Surg. 2013;29:364–366.
- Lambros V. Volumizing the brow with hyaluronic acid fillers. Aesthet Surg J. 2009;29:174–179.
- Glasgold M, Lam SM, Glasgold R. Volumetric rejuvenation of the periorbital region. Facial Plast Surg. 2010 Aug;26(3):252–259.