
Leon H. Kircik, MD; James Q. Del Rosso, DO, FAOCD; Daniel Aversa
Dr. Kircik is from Department of Dermatology, Indiana University Medical Center, Indianapolis, Indiana;
Department of Dermatology, Mount Sinai Medical Center, New York, New York, DermResearch, PLLC, Louisville, Kentucky.
Dr. Del Rosso is from Section of Dermatology ,Valley Hospital Medical Center, Las Vegas, Nevada; Las Vegas Skin and Cancer Clinics, Las Vegas, Nevada and Henderson, Nevada. Mr. Aversa is from Promius Pharma, LLC, Bridgewater, New Jersey
Disclosure: Drs. Kircik and DelRosso are consultants or speakers for Promius Pharma, LLC, the distributors of EpiCeram Emulsion. Daniel Aversa is a company employee. The manuscript describes a company-sponsored study (Promius Pharma, LLC, Bridgewater, New Jersey).
Abstract
Objectives: The objective of this study was to evaluate the efficacy of a ceramide-dominant, physiologic lipid-based topical emulsion, inclusive of ceramides, cholesterol, and fatty acids in a 3:1:1 ratio, in the clinical practice setting in subjects with mild-to-moderate atopic dermatitis. The included subjects presented with a wide range of demographic characteristics thus building upon the results reported with this agent from an earlier clinical trial in atopic dermatitis subjects. In addition, the utility of this important treatment approach of starting with a product directed at epidermal barrier repair was explored. Methods: In a 50-center, open-label, interventional study, the ceramide-dominant, physiologic lipid barrier repair emulsion was evaluated for three weeks in 207 patients either as monotherapy or in combination with another atopic dermatitis treatment. Outcome measures included investigator global assessment, investigator and subject satisfaction, subject-perceived improvement in atopic dermatitis, pruritus severity, and two quality-of-life questions. Results: Overall, approximately half of the subjects achieved success with investigator global assessment (clear or almost clear investigator global assessment scores) after three weeks of treatment with the ceramide-dominant, physiologic lipid barrier repair emulsion as monotherapy or in combination with another treatment. A large proportion of subjects (75% of subjects) and investigators (for 77% of subjects) reported satisfaction after three weeks of treatment. Pruritus and quality of life improved during the study. Conclusion: The ceramide-dominant, physiologic lipid-based product was shown to be an effective agent, with or without additional topical therapy, to provide good clinical efficacy and high levels of investigator and patient satisfaction for many patients with mild-to-moderate atopic dermatitis. The results of this study are consistent with results noted in a previous study of atopic dermatitis patients using this same barrier repair agent. The treatment approach of using a skin barrier repair cream as an integral and standard component of initial atopic dermatitis therapy, either as monotherapy or as a part of combination topical therapy, is supported by the outcomes observed in this study. This specific ceramide-dominant, physiologic lipid-based product may be used when initiating topical therapy for atopic dermatitis based on results from this and other studies.
(J Clin Aesthet Dermatol. 2011;4(3):34–40.)
Atopic dermatitis (AD) is a chronic-recurrent inflammatory skin disease that usually starts in early infancy and is characterized by pruritus. In the United States, the prevalence rate of AD is 10 to 12 percent in children and approximately one percent in adults.[1] A number of studies have reported that the financial burden to families and government is similar to that of asthma, arthritis, and diabetes mellitus. Among children with AD, the disease often causes significant psychological burden and a significant loss of school days.
Although the pathophysiology of AD is not fully understood, it is known to be characterized by a complex interaction of immunology, genetics, and skin barrier dysfunction.[2] While earlier treatment approaches primarily emphasized the suppression of Th2-mediated inflammation and pruritus, current treatment models also incorporate the importance of reversing epidermal barrier dysfunction, a major factor in the pathogenesis of AD. As a result, skin barrier repair is an essential part of the management of AD.
An updated treatment approach for AD, based on the “Outside-In” theory,[3] suggests that every AD patient requires application of an optimized epidermal barrier repair agent as an integral component of treatment. Other topical treatments, such as corticosteroids or immunomodulators, are also incorporated to maximize and expedite the reduction of visible eczematous inflammation and the associated symptoms that occur during active flares. For patients with mild eczematous disease, treatment with a well-formulated skin barrier repair agent as monotherapy may be sufficient, while patients with moderate or severe AD typically require a combination therapy approach. Combination treatment of AD includes a gentle skin cleanser, a skin barrier repair product, and usually a topical corticosteroid of adequate potency based on disease severity. Other alternatives include topical calcineurin inhibitors and sometimes more aggressive systemic treatment, including systemic therapy for severe or refractory disease. In clinical practice, multiple products are often prescribed, which may lead the patient to determine the actual need or desire for combination therapy. It is important that the patient be educated regarding the significance of each agent recommended for use in the combination regimen, why it is being selected, and when and how it should be used. Otherwise, many patients will be less likely to adhere to the complete regimen, thus leading to treatment failure.
A specific ceramide-dominant, physiologic lipid-based barrier repair emulsion (EpiCeram® Skin Barrier Emulsion, Promius Pharma, LLC) is a United States Food and Drug Administration (FDA)-cleared topical prescription product that is steroid-free, fragrance-free, and ceramide dominant. The product is indicated for the treatment of dry skin conditions and to manage and relieve the burning and itching associated with various types of dermatological conditions including AD, irritant contact dermatitis, and radiation dermatitis. This ceramide-dominant, physiologic lipid-based product has a 3:1:1 molar ratio of ceramides, cholesterol, and free fatty acids, which has been determined to be an optimal ratio to help skin barrier repair.[4] This ratio simulates the relative amount of these same three lipid components in the endogenous intercellular lipid membrane of the stratum corneum. This barrier repair product has demonstrated an excellent safety profile with no known significant risks. Occasional transient tingling upon application has been noted. This barrier repair agent can be used for all age groups, without restrictions for use on any cutaneous anatomical locations, such as the face or intertriginous areas. In addition, there is no recommended limitation on the duration of treatment time.
The efficacy of the ceramide-dominant, physiologic lipid-based product for the treatment of AD has been previously demonstrated in a prospective, randomized, controlled, investigator-blind, clinical trial. In this pivotal study, efficacy was compared to fluticasone propionate cream 0.05% in pediatric patients with moderate-to-severe AD.5 After four weeks of treatment, the ceramide-dominant, physiologic lipid-based emulsion showed comparable efficacy to fluticasone propionate 0.05% after two weeks and four weeks of treatment, both for the amelioration of pruritus and for improvement in sleep habits.
The objective of this more recent community-based study was to expand upon the results reported earlier by evaluating the efficacy of the ceramide-dominant, physiologic lipid-based product in real-world outpatient dermatology practice. This study setting included subjects with a wide range of demographic characteristics, all presenting with AD of mild-to-moderate severity. The protocol design was a multicenter, open-label, interventional study evaluating the ceramide-dominant, physiologic lipid-based product, either as monotherapy or as part of combination topical therapy in subjects with mild-to-moderate AD, with the choice of approach determined by patients (parents or guardians where applicable). The duration of treatment was three weeks. Use of community-based medical practices rather than formal clinical research centers in this study provided response data as determined “through the eyes of the practicing clinical dermatologist,” which can elicit a different, yet clinically relevant perspective as compared to investigators who are only employed at a research center. Although some subjects used combination topical therapy, this report focuses on overall results for all subjects since there was no difference in efficacy between combination topical therapy and monotherapy. Subgroup analyses are planned for future publications.
Materials and Methods
Study parameters. This study was an open-label, community-based trial conducted at 50 sites in the United States. Investigators for the study were required to be licensed dermatologists in the state where the study was being conducted. Investigators had a community-based medical practice and were required to see a large number of patients with mild-to-moderate AD in order to ensure rapid completion of enrollment. The study protocol and informed consent form were approved by an institutional review board operating in compliance with federal regulations. Subjects of all ages and races with mild-to-moderate AD on the investigator global assessment (IGA) scale were eligible for enrollment. Mild-to-moderate AD on the IGA scale was defined as mainly very light pink to dull red lesions, with or without barely to clearly perceptible elevation, with up to some oozing and crusting. Any current medication for AD was discontinued upon study enrollment, and subjects could not have had any prior treatment with the designated study product (ceramide-dominant, physiologic lipid-based emulsion). Demographic data was collected including age, race, sex, skin type, location of AD, flare frequency, year diagnosed, related medical conditions (seasonal rhinitis, asthma, and/or food allergies), family history of AD, alcohol consumption, and tobacco use.
Subjects were instructed to apply the designated barrier repair study product (ceramide-dominant, physiologic lipid-based emulsion) to affected areas and commonly involved sites of AD (e.g., antecubital region, popliteal region) twice daily, approximately every 12 hours, for a duration of three weeks. Subjects were also given a prescription for another AD medication, chosen by the investigator, and instructed to use this medication along with the ceramide-dominant, physiologic lipid-based product, as combination therapy, only if their condition worsened significantly and was not adequately controlled by the barrier repair study product alone.
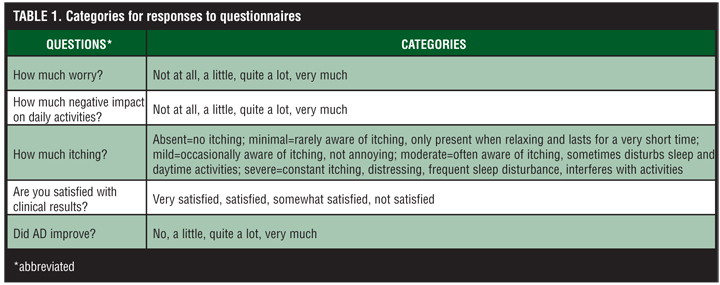
At baseline and at the Week 3 visit, the investigator assessed the severity of AD using the IGA scale (0=clear, 1=almost clear, 2=mild, 3=moderate, 4=severe) and subjects rated severity of pruritus. Quality of life (QOL) was also assessed at both visits regarding general worry and negative impact on daily activities. At the Week 3 visit, subjects reported their perceived improvement, satisfaction, adverse events, adherence to study treatment and need for the prescribed medication. Investigators also reported their satisfaction with the clinical results at Week 3. Categories for responses to questions about quality of life, pruritus, and satisfaction are shown in Table 1.
{kind=link}
Statistical methods. All statistical analyses were performed on the ITT data set at the 0.05 alpha level, two tailed. The primary efficacy variable was the change from Baseline in IGA at Week 3. A paired-t test was used to analyze the change from Baseline. IGA was also dichotomized as success (clear or almost clear) and failure, and the proportion of subjects with IGA success were summarized. Other variables were also dichotomized. For categorical variables, chi-square test or McNemar test was used, as appropriate.
Results
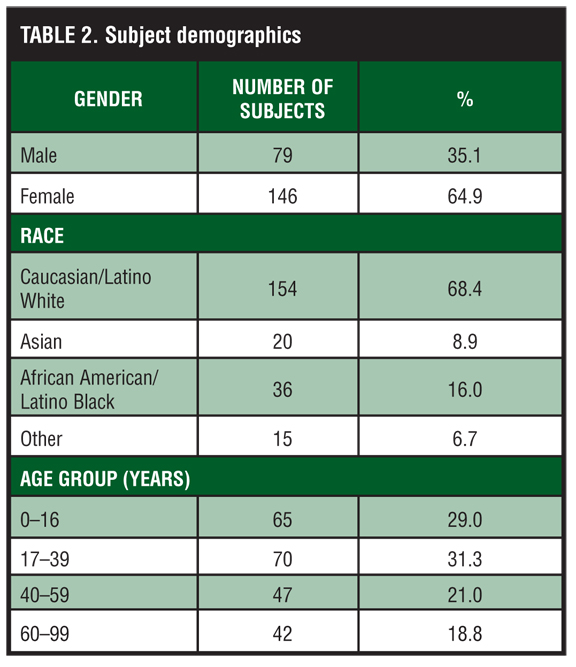
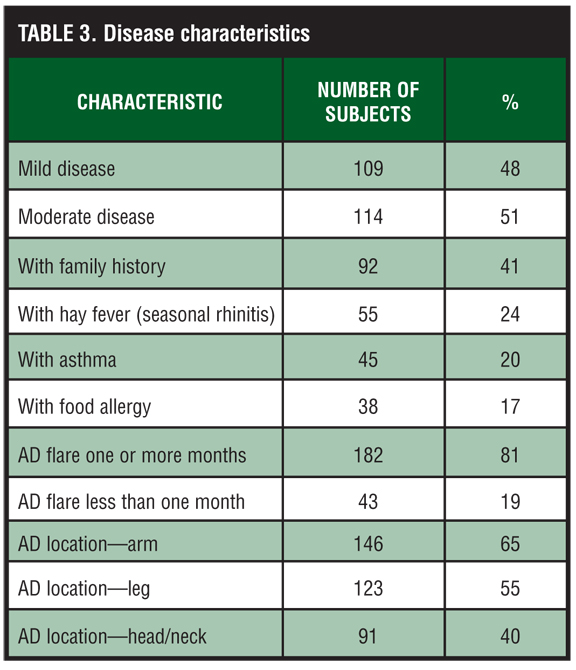
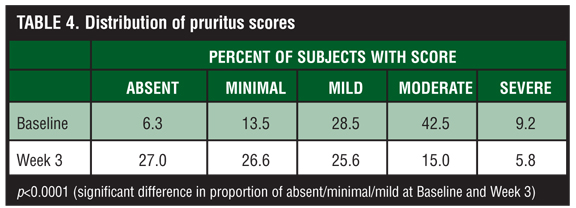
Subject characteristics. Informed consent was obtained for 225 subjects enrolled from August 2009 to February 2010, and 207 subjects completed the study. At the end of the study, 17 subjects were lost to follow up and one subject withdrew consent. The demographic characteristics of the subjects are shown in Table 2. Disease characteristics are summarized in Table 3. Subjects initially had mild-to-moderate AD, some with no pruritus (6%) and some with severe pruritus (9%) (Table 4). The majority of subjects were female (65%) and Caucasian (68%) with a mean age of 34 years (3 months to 93 years). Subjects with a range of Fitzpatrick skin types from I to VI were well represented. Most subjects were nonsmokers (91%) and either denied alcohol use or rarely consumed alcoholic drinks (78%). Immediate family members had a history of AD for 41 percent of subjects, most often the mother or father. Half of the subjects had no associated conditions while 24 percent had seasonal rhinitis (hay fever), 20 percent had asthma, and 17 percent had food allergies. The median duration of diagnosis of AD was five years (less than 1 to 83 years). Among this subject population, AD flares were historically frequent with 81 percent of subjects reporting that their AD flared one or more times a month versus 19 percent of subjects who reported flaring less than one time per month. The most common locations of disease were on the arms (65% of subjects) and legs (55%).
{kind=link}
{kind=link}
{kind=link}
One hundred forty-eight subjects (72%) used the ceramide-dominant, physiologic lipid-based emulsion every day of the study, while 45 subjects (22%) used it “most every day” and 14 subjects (7%) used it “occasionally.” The majority of subjects, 147 subjects (71%), did not use the prescribed additional medication and completed the entire three weeks of the study using only the ceramide-dominant, physiologic lipid-based emulsion (monotherapy). Sixty subjects (29%) used combination topical therapy (ceramide-dominant, physiologic lipid-based emulsion plus the prescribed medication). Subjects who used the prescribed medication used it an average of 8.4 days during the study. The other prescribed topical treatments that were used were predominantly topical corticosteroids (low, mid and high potency) with a few subjects using tacrolimus ointment (three subjects). The vast majority of subjects who ultimately utilized combination therapy used topical agents only; however, two subjects used an oral antihistamine as the additional prescribed treatment. Interestingly, there was no difference in the number of subjects who used combination therapy between study groups with mild and moderate IGA at Baseline (p>0.05).
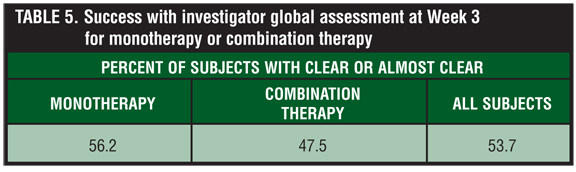
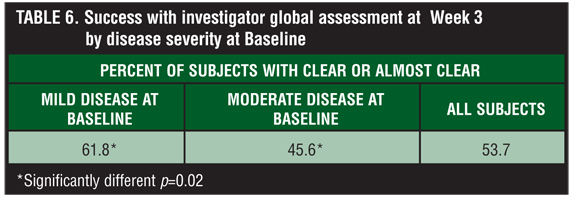
Efficacy results. Fifty-four percent of all subjects were clear or almost clear at Week 3, and thus were rated as “treatment success” based on IGA. Table 5 displays a categorical analysis of subjects with success for IGA at Week 3 by disease severity at Baseline, and Table 6 shows the results for combination therapy (almost always topical only in this study) versus monotherapy. A statistically significantly greater proportion of subjects with mild disease at Baseline had success compared to subjects with moderate disease (62% vs. 46%, p=0.02). There were no statistical differences in success rate between the combination therapy and monotherapy groups. The mean IGA at Baseline was 2.49, which was statistically significantly reduced by an average of 40 percent to a mean of 1.47 at Week 3 (p<0.001).
{kind=link}
{kind=link}
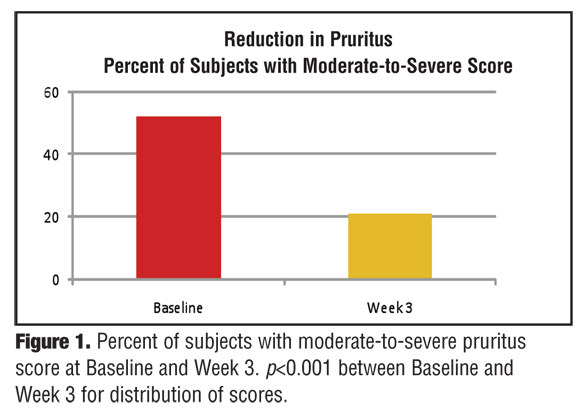
The severity of pruritus experienced during the previous 24-hour period as reported by study subjects decreased significantly (p<0.001) from Baseline to Week 3. At baseline, 52 percent of subjects reported moderate or severe pruritus during the previous 24-hour period (Table 4). At Week 3, subjects reporting moderate or severe pruritus decreased to 21 percent (Table 3, Figure 1). Overall, 69 percent of subjects with mild, moderate, or severe pruritus at Baseline reported less pruritus at Week 3. The mean pruritus score at Baseline was 2.35 compared to 1.46 at Week 3, reflecting an average reduction of 38 percent.
{kind=link}
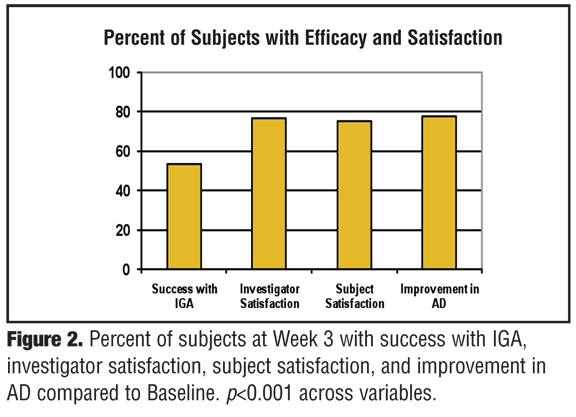
Satisfaction with clinical results. Figure 2 displays success with IGA alongside satisfaction results for all subjects and shows that the overall level of satisfaction and perceived improvement were statistically significantly higher than IGA scoring (p<0.001). For 77 percent of subjects, the investigators were satisfied (very satisfied= 38%, satisfied=24%, or somewhat satisfied=14%) with the clinical results observed for the subject at Week 3, and 75% of subjects were satisfied (39%, 18%, 18%, respectively) with their clinical results as compared to Baseline. Seventy-eight percent of subjects believed that their AD had improved, at least a little, since Baseline.
{kind=link}
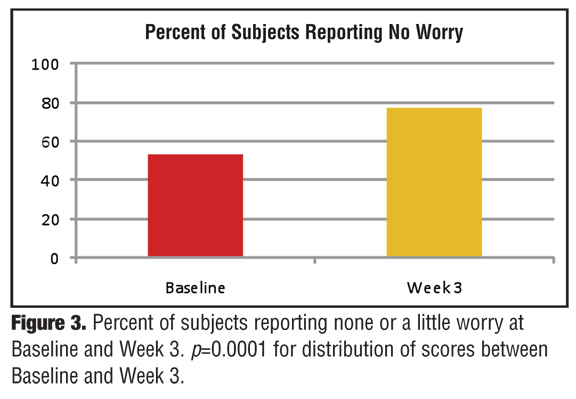
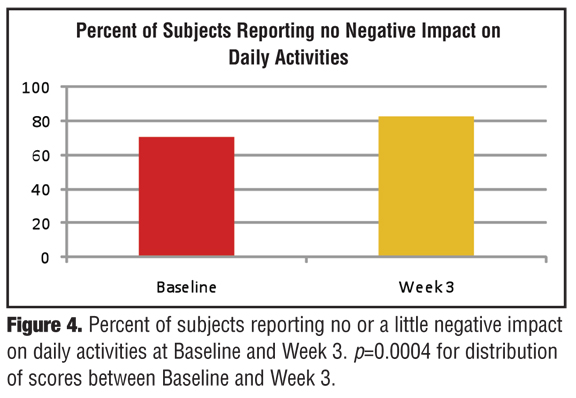
Quality-of-life assessments. Subjects were asked to rate “worry” about their AD and the negative impact on daily activity at Baseline and Week 3 using two questions. After using the ceramide-dominant, physiologic lipid-based emulsion for three weeks, 77 percent of subjects reported no (34%) or a little worry (43%) about their AD compared to 53 percent at Baseline (p<0.0001) (Figure 3). Significantly more subjects (p=0.0004) reported no or minimal negative impact on daily activities after three weeks of using the ceramide-dominant, physiologic lipid-based emulsion treatment compared to Baseline (83% vs. 71%) (Figure 4).
{kind=link}
{kind=link}
Adverse events. Six subjects (3%) reported a total of seven related, mild or moderate adverse events (AEs). An additional nine subjects reported worsening of AD that was considered an AE. AEs related to study treatment included erythema, skin irritation, pruritus, paresthesia, and pain. One worsening of AD was rated as severe and one subject had severe acarodermatitis (tick bite). There were no serious AEs.
Discussion
The objective of this study was to evaluate the efficacy, tolerability and level of satisfaction associated with use of a ceramide-dominant, physiologic lipid-based topical emulsion in the setting of ambulatory dermatology practice for patients with mild-to-moderate AD. Fifty dermatologists from community-based medical practices enrolled 225 subjects and provided data from the perspective of the practicing clinical dermatologist. Subjects presented with a wide range of demographic characteristics. The youngest subject was three-months old with a recent diagnosis of AD, while the oldest subject was 93 years old with an 83-year history of AD. Most subjects were nonsmokers with some modest diversity in the reported consumption of alcoholic beverages. Half of the subjects did not report conditions commonly associated with AD, specifically seasonal rhinitis, asthma, and food allergies.
Unique to this study was the direct involvement of subjects in deciding whether to use an additional treatment in combination with the ceramide-dominant, physiologic lipid-based emulsion. At the Baseline visit, subjects were given a tube of the ceramide-dominant, physiologic lipid-based emulsion to use immediately and a prescription chosen by the investigator for an additional AD treatment, to be used at the discretion of the subject based on his or her assessment of response to the ceramide-dominant, physiologic lipid-based product or other factors, such as the requirement of the subject to buy the product. The majority of subjects (71%) chose not to use the prescribed additional medication and used only the ceramide-dominant, physiologic lipid-based product during the three-week study period.
Overall, approximately half of the subjects achieved “treatment success” based on IGA (clear or almost clear IGA scores) after three weeks of treatment with the ceramide-dominant, physiologic lipid-based emulsion either as monotherapy (56% of subjects had success), or in combination with another treatment (47% of subjects had success). Since the combination product was not standardized with regard to potency, vehicle, or active component or treatment regimen, conclusions about the improvement of subjects using the combination product along with the ceramide-dominant, physiologic lipid-based emulsion are difficult.
A high level of satisfaction with the clinical results was noted both by subjects (75% of subjects) and investigators (for 77% of subjects) after three weeks of treatment. In this study it appears that clinical efficacy alone did not contribute to satisfaction, as rates of satisfaction were higher than the rates reported for clinical success.
This study illustrates the utility of a brand ceramide-dominant, physiologic lipid-based emulsion in the clinical practice setting using a topical treatment approach, which immediately incorporates an epidermal barrier repair product. This approach is based on the “Outside-In” theory of AD. The “Outside-In” theory suggests that patients with mild AD may be controlled with the use of a well-formulated skin barrier repair product alone, while patients with moderate or more severe disease may require combination therapy, often warranting use of a potent anti-inflammatory agent, such as a topical corticosteroid. Since most subjects chose not to use combination therapy, it was not surprising that more subjects with mild disease achieved IGA success (62%) compared to subjects with moderate disease (46%). Interestingly, Baseline severity did not influence whether or not combination therapy was used by the patient. No guidance was given to investigators about how to instruct subjects on the treatment plan and the requirement for subjects to purchase the additional medication may have played a role in the number of patients opting for monotherapy. However, the study was designed to simulate real-world clinical practice as closely as possible and typically patients must choose whether or not to purchase multiple medications prescribed by the physician.
This study was also open label and not placebo controlled, which may have influenced success rates to some degree. In addition, satisfaction was not specifically defined in the protocol and analysis of factors that correlate with satisfaction could identify important considerations that drive whether or not patients are pleased with their therapy. Importantly, the subjects decided on their own whether or not to use the additional treatment.
In conclusion, a brand ceramide-dominant, physiologic lipid-based topical emulsion was shown to be an effective agent that can be used with or without additional AD therapy to provide good clinical efficacy and high levels of investigator and patient satisfaction for the treatment of mild-to-moderate AD. These results serve to further validate the good efficacy seen in an earlier study with ceramide-dominant, physiologic lipid-based emulsion in subjects with AD. This study also supports a currently accepted treatment approach of using a targeted skin barrier repair product for all AD patients to address the underlying defective skin barrier inherent to AD. Additional prescription products may be incorporated to expedite the reduction of cutaneous inflammation and associated symptoms for patients with AD, especially when disease is greater in severity. In particular, the ceramide-dominant, physiologic lipid-based emulsion evaluated in this study was found to be an effective product to use initially in the management of AD and may be sufficient as monotherapy in many patients with mild-to-moderate disease.
Acknowledgments
The authors wish to acknowledge the EPIC study group: Anderson, Yonkers, New York; Appell, Birmingham, Alabama; Bettencourt, Henderson, Nevada; Borenstein, P. B. G., Florida; Boucher, San Antonio, Texas; Braun, Uniontown, Pennsylvania; Castellano, Sher. Oaks, California; Chew, Columbia, Maryland; Cohen, Macon, Georgia; Cooper, Tucker, Georgia; Davis, San Antonio, Texas; Duke, Mystic, Connecticut; Fleischman, Leawood, Kansas; Forsha, West Jordan, Utah; Fujita, Aiea, Hawaii; Gin, Los Gatos, California; Gold, Nashville, Tennesee; Guagenti, Glendale, California; Ha, Roseville, California; Hruza, St. Louis, Missouri; Jacobson, Hoover, Alabama; Kayal, Marietta, Georgia; Kerdel, Miami, Florida; Kleinman, Burlington, North Carolina; Kodama, Puyallup, Washington; Kozeny, Buffalo Grove, Illinois; Knuckles, Corbin, Kentucky; Lerman, Bronx, New York; McCune, Overland Pk, Kansas; Oyler, Raleigh, North Carolina; Poole, Metaire, Lousiana; Press, Fresno, California; Rabner, West Caldwell, New Jersey; Ratoosh, Pasadena, Texas; Rhodes, Ridley Park, Pennsylvania; Scannon, Tampa, Flordia; Scheinfeld, New York, New York; Schmeider, Orange Pk, Florida; Schoenfeld, Carrollton, Georgia; Schwat, San Francisco, California; Silverberg, Brooklyn, New York; Silverton, Grand Blanc, Michigan; Smith, Vineland, New Jersey; Smith, Louisville, Kentucky; Strobel, Catonsville, Maryland; Taylor, Philadelphia, Pennsylvania; Turner, Memphis, Tennesee; Waldman, Charlotte, North Carolina; Wikas, Cuyahoga Falls, Ohio; Zaiac, Miami Beach, Florida.
References
1. Kligman LH, Kligman AM. The nature of photoaging: its prevention and repair. Photodermatol. 1986;3:215–227.
2. El-Domyati M, Attia S, Saleh F, et al. Intrinsic aging vs. photoaging: a comparative histopathological, immuno-histochemical, and ultrastructural study of skin. Exp Dermatol. 2002;11:398–405.
3. Helfrich YR, Sachs DL, Voorhees JJ. Overview of skin aging and photoaging. Dermatol Nurs. 2008;20:177–183.
4. Uitto J. The role of elastin and collagen in cutaneous aging: intrinsic aging versus photoexposure. J Drugs Dermatol. 2008;7:S12–S16.
5. Sadick NS, Weiss R. Intense pulsed-light photorejuvenation. Semin Cutan Med Surg. 2002;21:280–287.
6. El-Domyati M, Attia S, Saleh F, et al. Effect of topical tretinoin on photoaged facial skin: a histometric, immunohistochemical and ultrastructural study. J Cosmet Dermatol. 2004;3: 191–201.
7. Kim KH, Geronemus RG. Nonablative laser and light therapies for skin rejuvenation. Arch Facial Plast Surg. 2004;6:398–409.
8. Sadick NS, Makino Y. Selective electro-thermolysis in aesthetic medicine: a review. Lasers Surg Med. 2004;34: 91–97.
9. Trelles MA, Allones I, Velez M. Nonablative facial skin photorejuvenation with an intense pulsed light system and adjunctive epidermal care. Lasers Med Sci. 2003;18:104–111.
10. Bogle MA, Ubelhoer N, Weiss RA, et al. Evaluation of the multiple pass, low fluence algorithm for radiofrequency tightening of the lower face. Lasers Surg Med. 2007;39: 210–217.
11. Kist D, Burns AJ, Sanner R, et al. Ultrastructural evaluation of multiple pass low energy versus single pass high energy radio-frequency treatment. Lasers Surg Med. 2006;38: 150–154.
12. Glogau RG, Matarasso SL. Chemical peels. Trichloroacetic acid and phenol. Dermatol Clin. 1995;13:263–276.
13. Mahoney MG, Brennan D, Starcher B, et al. Extracellular matrix in cutaneous aging: the effects of 0.1% copper-zinc malonate-containing cream on elastin biosynthesis. Exp Dermatol. 2009;18:205–211.
14. Whittaker P, Kloner RA, Boughner DR, et al. Quantitative assessment of myocardial collagen with picrosirius red staining and circularly polarized light. Basic Res Cardiol. 1994;89:397–410.
15. Rich L, Whittaker P. Collagen and picrosirius red staining: a polarized light assessment of fibrillar hue and spatial distribution. Braz J Morphol Sci. 2005;22:97–104.
16. Chung HJ, Uitto J. Type VII collagen: the anchoring fibril protein at fault in dystrophic epidermolysis bullosa. Dermatol Clin. 2010;28:93–105.
17. Watson RE, Ball SG, Craven NM, et al. Distribution and expression of type VI collagen in photoaged skin. Br J Dermatol. 2001;144:751–759.
18. Villone D, Fritsch A, Koch M, et al. Supramolecular interactions in the dermo-epidermal junction zone: anchoring fibril-collagen VII tightly binds to banded collagen fibrils. J Biol Chem. 2008;283:206–213.
19. Amano S. Possible involvement of basement membrane damage in skin photoaging. J Investig Dermatol Symp Proc. 2009;14:2–7.
20. Mezzana P, Valeriani M. Rejuvenation of the aging faces using fractional photothermolysis and intense pulsed light: a new technique. Acta Chir Plast. 2007;29:47–50.
21. Nelson JS, Majaron B, Kelly KM. What is nonablative photorejuvenation of human skin? Semin Cutan Med Surg. 2002;21:238–250.
22. DeHoratius DM, Dover JS. Nonablative tissue remodeling and photorejuvenation. Clin Dermatol. 2007;25:474–479.
23. Goldberg DJ, Rogachefsky AS, Silapunt S. Non-ablative laser treatment of facial rhytides. A comparison of 1450 nm diode laser treatment with dynamic cooling device as opposed to treatment with dynamic cooling alone. Lasers Surg Med. 2002;30:79–81.
24. Fournier N, Dahan S, Barneon G, et al. Nonablative remodeling: clinical, histologic, ultrasound imaging, and profilometric evaluation of a 1540nm Er:glass laser. Dermatol Surg. 2001;27:799–806.
25. Grema H, Greve B , Raulin C. Facial rhytides—subsurfacing or resurfacing? A review. Lasers Surg Med. 2003;32: 405–412.
26. Sadick NS, Alexiades-Armenakas M, Bitter PJ, et al. Enhanced full-face skin rejuvenation using synchronous intense pulsed optical and conducted bipolar radiofrequency energy (ELOS): introducing selective radiophotothermolysis. J Drugs Dermatol. 2005;4:181–186.
27. Bitter PJ, Stephen Mulholland R. Report of a new technique for enhanced non-invasive skin rejuvenation using a dual mode pulsed light and radio-frequency energy source: selective radio-thermolysis. J Cosmet Dermatol. 2002;1: 142–143.
28. Hammes S, Greve B, Raulin C. Electro-optical synergy (ELOS) technology for non-ablative skin rejuvenation: a preliminary prospective study. J Eur Acad Dermatol Venereol. 2006;20:1070–1075.
29. Ruiz-Esparza J, Gomez JB. Nonablative radiofrequency for active acne vulgaris: the use of deep dermal heat in the treatment of moderate-to-severe active acne vulgaris (thermotherapy): a report of 22 patients. Dermatol Surg. 2003;29:333–339.
30. El-Domyati M, Attia S, Saleh F, et al. Trichloroacetic acid peeling versus dermabrasion: a histometric, immuno-histochemical, and ultrastructural comparison. Dermatol Surg. 2004;30:179–188.
31. Ruiz-Esparza J. Nonablative radiofrequency for facial and neck rejuvenation. A faster, safer, and less painful procedure based on concentrating the heat in key areas: the ThermaLift concept. J Cosmet Dermatol. 2006;5:68–75.
32. Doshi SN, Alster TS. Combination radiofrequency and diode laser for treatment of facial rhytides and skin laxity. J Cosmet Laser Ther. 2005;7:11–15.