
 by Joshua A. Zeichner, MD; Lawrence F. Eichenfield, MD; Steven R. Feldman, MD, PhD; J. Scott Kasteler, MD; and Ilia L. Ferrusi, PhD
by Joshua A. Zeichner, MD; Lawrence F. Eichenfield, MD; Steven R. Feldman, MD, PhD; J. Scott Kasteler, MD; and Ilia L. Ferrusi, PhD
Dr. Zeichner is with Mount Sinai Hospital in New York, New York. Dr. Eichenfield is with the University of California and Rady Children’s Hospital, both in San Diego, California. Dr. Feldman is with the Wake Forest University School of Medicine in Winston-Salem, North Carolina. Dr. Kasteler is with the University of Louisville in Louisville, Kentucky. Dr. Ferrusi is with Allergan plc in Irvine, California.
Funding: This study was sponsored by Allergan plc (Dublin, Ireland).
Disclosures: Dr. Zeichner has been an advisory board member, consultant, or speaker for Allergan, Bayer, Foamix, Galderma, Intraderm, Isdin, Janssen, Johnson and Johnson, L’Oreal, Novan, and Promius. Dr. Eichenfield has been a consultant and investigator for Allergan, Galderma, Novan, and Valeant. Dr. Feldman has been an investigator, speaker, and/or consultant for Abbvie, Advance Medical, Caremark, Celgene, Galderma, Janssen, Kikaku, Leo Pharma, Lilly, Merck, Mylan, Novartis, Pfizer, Qurient, Sanofi, Sienna, Sun Pharmaceuticals, Suncare Research, Taro, Valeant, and Xenoport. Dr. Feldman also owns stock in Causa Technologies and Medical Quality Enhancement Corporation, has received royalties from Informa, UpToDate, and Xlibris, and is Founder and Chief Technology Officer of Causa Technologies. Dr. Kasteler has been an investigator and a speaker for Allergan, Amgen, Bayer, Novartis, and Sun Pharmaceuticals, and has participated in advisory board meetings for Amgen, Bayer, and Sun Pharmaceuticals. Dr. Ferrusi was an employee of Allergan plc at the time the study was conducted.
Abstract: Objective. The objective of the study was to evaluate the impact of rosacea on self-perception, emotional, social, and overall well-being and quality of life in individuals with erythematotelangiectatic rosacea (ETR) and papulopustular rosacea (PPR).
Design. We distributed a cross-sectional email invitation for participants in the United States to fill out a web-based survey.
Participants. We included adults who reported having previously received a diagnosis of erythematotelangiectatic rosacea or papulopustular rosacea.
Measurements. Questionnaires measured the psychosocial aspects of rosacea, including the Satisfaction With Appearance Scale and modified Satisfaction With Appearance Scale questionnaires, Impact Assessment for Rosacea Facial Redness, Rosacea-Specific Quality-of-Life questionnaire, and RAND 36-Item Short Form Health Survey. The Impact Assessment for Rosacea Facial Bumps or Pimples was administered to the papulopustular rosacea cohort.
Results. Six hundred participants enrolled and completed the survey, with most rating their rosacea as mild or moderate (ETR: 95.6%; PPR: 93.7%). In the erythematotelangiectatic rosacea and papulopustular rosacea cohorts, respectively, 45 and 53 percent disagreed/strongly disagreed that they were satisfied with their appearance due to rosacea; 42 and 27 percent agreed/strongly agreed that they “worry how people will react when they see my rosacea”; and 43 and 59 percent agreed/strongly agreed that they feel their rosacea is unattractive to others. Rosacea-Specific Quality-of-Life total and domain scores indicated negative impact of rosacea for both cohorts. Both cohorts reported worse 36-item Short Form Health Survey overall and domain scores than population norms in the United States.
Conclusion. Rosacea had wide-ranging, negative effects on self-perceptions and emotional, social, and overall well-being as well as rosacea-specific quality of life. Overall, both erythematotelangiectatic rosacea and papulopustular rosacea cohorts reported a substantial negative impact of rosacea on quality of life on a range of instruments.
Keywords: Rosacea; erythematotelangiectatic rosacea; papulopustular rosacea; quality of life; psychosocial impact
J Clin Aesthet Dermatol. 2018;11(2):47–52
Introduction
Rosacea is a chronic disorder characterized by persistent centrofacial erythema that affects approximately 16 million adults in the United States (US).1–3 There are several subtypes of rosacea, the most common of which is erythematotelangiectatic rosacea (ETR).1 ETR is typified by persistent centrofacial erythema and flushing with the presence or absence of telangiectases.4 The second most common subtype of rosacea is papulopustular rosacea (PPR), which consists of persistent centrofacial erythema along with transient, central facial papules and/or pustules.1,4
The pathophysiology of rosacea is not completely understood. However, data suggest the involvement of an abnormally functioning innate immune detection and response system, which induces activation of inflammatory cascades.1,4 Vasodilation, an outcome of neurovascular dysregulation, has also been implicated in the pathogenesis of rosacea.5 In addition to the symptomatic effects of rosacea, the condition can have a substantial psychosocial impact and substantial effects on quality of life (QoL). To that end, rosacea might have a considerable impact on the lives of patients, including negative effects on self-esteem and self-confidence along with decreased QoL.6–11
The objective of this cross-sectional survey was to assess the burden of illness associated with rosacea. A previous report from this study included analyses of sociodemographics, symptoms, treatment utilization, and satisfaction with treatment.12 These analyses demonstrated an overall lack of satisfaction with the treatments available for rosacea, coupled with a low level of treatment utilization. These results indicated that while treatment might be effective in the short term, participants do not continue with use of specific treatments, resulting in intermittent use and low treatment satisfaction. Here, we describe the impact of rosacea symptoms on self-perception, emotional, social, and overall well-being, and rosacea-specific QoL in individuals with ETR and PPR subtypes.
Methods
Details of the conduct of this study have been described previously.12
This was a cross-sectional, web-based survey administered over a two-month time period to adults in the United States. Ethical approval for the study was obtained from the Chesapeake Institutional Review Board (Columbia, Maryland) in compliance with regulatory guidelines and in accordance with requirements of studies involving human respondents. Survey respondents provided informed consent via a web-linked opt-in process before starting any study activities. United BioSource Corporation (Bluebell, Pennsylvania) monitored the conduct of the survey, which was administered by Ipsos Observer (Paris, France). The survey was conducted between May 8, 2015, and July 1, 2015.
Prospective participants completed an eligibility survey designed to identify those with a prior rosacea diagnosis and current erythema. Participants were asked to rate the severity of their erythema using a scale designed to assess facial redness associated with rosacea. Eligible participants were male or female adults age 18 years or older who self-reported having received a physician’s diagnosis of rosacea at any time in the past, were able to read and understand English, and provided informed consent. Exclusion criteria included self-rated facial redness that was less than “mild” at the time of the survey based on the validated Subject Self-Assessment for Rosacea Facial Redness scale with photo guide or any of the following covering more than 25 percent of the face: telangiectases (visible blood vessels), sun-damaged skin (irregular coloring or pigmentation of the skin, with a mottled, wrinkled appearance and liver spots or age spots), or acne.
Participants who completed the survey and indicated the presence of at least mild facial redness were classified into an ETR or a PPR cohort, based on the presence of four or more inflammatory bumps or pimples at the time of survey completion (PPR). In the ETR cohort, severity was assessed using the Subject Self-Assessment for Rosacea Facial Redness scale with photo guide, while in the PPR cohort severity was categorized based on the number of facial lesions alone. Participants who indicated having 4 to 9 facial bumps or pimples were classified as having mild PPR, 10 to 20 as moderate PPR, and 21 or more as severe PPR.
Participants answered questions about attitudes, self-perception, and satisfaction with appearance as a result of rosacea. Questions on satisfaction with appearance were modeled after the Satisfaction With Appearance Scale (SWAP) questionnaire validated for burn patients13 and after the modified SWAP questionnaire, adapted and validated for patients with systemic sclerosis.14 A number of different questionnaires were also administered to the participants to assess the impact of rosacea on QoL. The Impact Assessment for Rosacea Facial Redness (IA-RFR), an instrument developed and validated by Allergan plc (Dublin, Ireland) based on standards recommended by the United States Food and Drug Administration (FDA) to measure patient-reported outcomes, was administered to all participants.15 The IA-RFR consists of eight individual items within four domains (Self-perception, Emotional, Grooming, and Social) that were rated on a five-point adjectival scale from 0 (no negative impact) to 4 (greatest negative impact). The recall period for each item was seven days. The Impact Assessment for Rosacea Facial Bumps or Pimples (IA-RFB), an instrument adapted from the IA-RFR, was administered to participants in the PPR cohort only. The validated Rosacea-specific Quality-of-Life (RosaQoL) questionnaire, a 21-item instrument based on the 29-item version of the Skindex survey instrument,16,17 was also administered and includes Emotion, Symptom, and Function domains.18 The recall period for this scale was four weeks; response options were based on a five-point adjectival scale (1 = never; 5 = all the time), with higher domain scores indicating a greater level of burden.18 Finally, the RAND 36-Item Short Form Health Survey (SF-36) version 1.0 was used to assess health-related QoL across eight domains: Physical Functioning, Role Limitations Due to Physical Health (which the SF-36 refers to as Physical Role), Role Limitations Due to Emotional Problems (Emotional Role), Energy/Fatigue (Vitality), Emotional Well-being (Mental Health), Social Functioning, Pain (Bodily Pain), and General Health. The recall period for the scale was four weeks. SF-36 domain scores range from 0 to 100, with higher scores indicating better health status. SF-36 scores were compared with published SF-36 data from the general US population.19
Limited inferential analyses were conducted for key outcomes. Analyses were performed on the population of evaluable participants, which comprised eligible respondents who completed the survey in its entirety. For the IA-RFR and the adapted IA-RFB instruments, all items were transformed to a scale of 0 to 100. The range of scores was set to have the lowest response category set to zero, dividing by the value of the highest response category and then multiplying by 100. Domain scores were calculated as the average of the transformed scores for items within the scale. For the RosaQoL instrument, within each domain, scores were the average of all responses to the items in the domain scale. Similarly, the total score was the average of all responses with individual scale scores weighted equally.
Results
A total of 600 eligible participants were enrolled and completed the survey, including 409 participants with ETR symptoms and 191 with PPR symptoms. Details of participant screening, disposition, and sociodemographics have been presented in a previous publication. Rosacea was self-rated as mild by 63.6 and 62.8 percent of participants in the ETR and PPR cohorts, respectively; fewer participants self-rated rosacea as moderate (ETR, 32.0% ; PPR, 30.9%). The mean age of participants was 53.1 years in the ETR cohort and 48.7 years in the PPR cohort. Body mass index (BMI) measurements indicated that, overall, 69.0 percent were classified as overweight or obese. Overall, approximately two-thirds of the participants were female; 95.7 percent were Caucasian. More than 99 percent had an education level of a high school diploma or higher, and more than 90 percent had private medical insurance and prescription drug coverage.
Participants in the ETR and PPR cohorts expressed dissatisfaction with their appearance and negative feelings about their appearance because of their rosacea symptoms (Table 1). A small proportion of subjects in either cohort agreed or strongly agreed that they were satisfied with their facial appearance due to rosacea (Table 1), and almost half (45%) of the ETR cohort and 53 percent of the PPR cohort disagreed or strongly disagreed that they were satisfied with their facial appearance due to rosacea.
A substantial proportion of participants in both cohorts indicated that they worry about how others perceive them based on their rosacea (Tables 1 and 2). Overall, both the ETR and PPR cohorts expressed negative views as to how others might perceive them; 27 percent of the ETR cohort and 42 percent of the PPR cohort agreed or strongly agreed that they worry how people would react to seeing their rosacea. Following the same pattern, 43 percent of the ETR cohort and 59 percent of the PPR cohort agreed or strongly agreed that their rosacea is unattractive to others. A total of 30 percent of the ETR cohort and 44 percent of the PPR cohort agreed or strongly agreed that they worry that people jump to false conclusions based on their facial redness. In addition, variable but substantial proportions of the ETR and PPR cohorts agreed or strongly agreed that they worry that others perceive them as less likely to be successful, confident, or have a romantic partner, and more likely to be shy or unhealthy (Table 2).
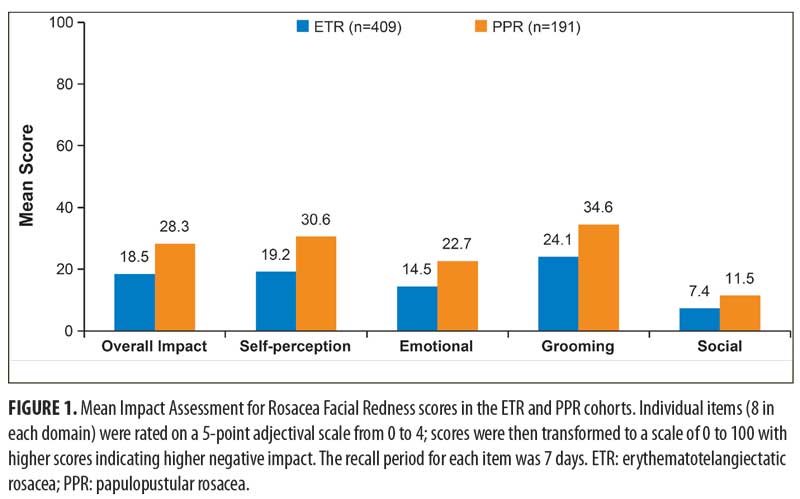
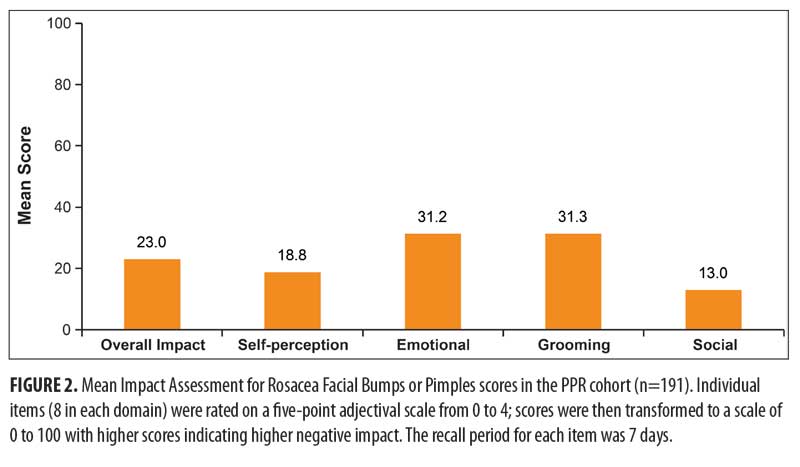
Rosacea facial redness had a negative impact on all study participants for all domains of the IA-RFR questionnaire (Figure 1). In the PPR cohort, bumps and pimples had the greatest negative impact in the Emotional and Grooming domains of the IA-RFB questionnaire (Figure 2). Notably, in the PPR cohort, comparison of the overall impact of facial redness (IA-RFR) and of bumps and pimples (IA-RFB) indicated that the negative impact of facial redness was numerically greater. A greater negative impact of facial redness was also observed in the Self-perception and Grooming domains. However, facial redness had a less negative impact than bumps and pimples in the Emotional and Social domains.
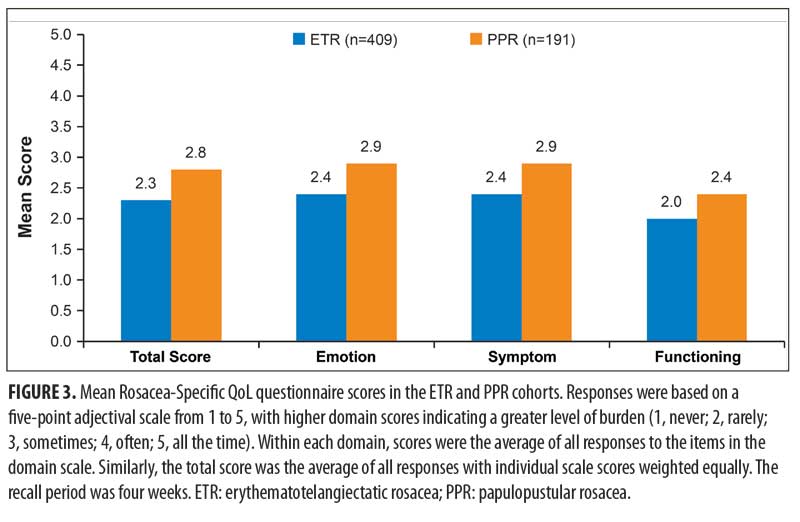
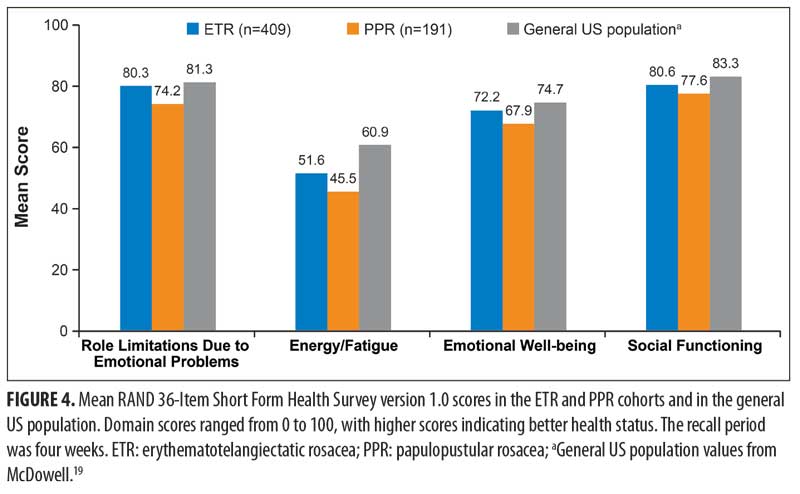
RosaQoL total scores and Emotion, Symptom, and Functioning domain scores were similar within each cohort, and ranged from 2.0 to 2.9, indicating responses of “rarely” to most of the questionnaire items (Figure 3). The PPR cohort had numerically higher mean scores than the ETR cohort overall and in all RosaQoL domains, suggesting that PPR might have a slightly greater negative impact on QoL than ETR. Results from the SF-36 questionnaire (Figure 4) showed that both the ETR and the PPR cohorts had lower scores than the US general population overall and for each individual domain within the questionnaire.19 Mean Role Limitations Due to Emotional Problems, Energy/Fatigue, Emotional Well-being, and Social Functioning scores were numerically lower in the PPR cohort than the ETR cohort.
Discussion
This comprehensive survey of a large cohort of individuals who reported a diagnosis of rosacea found that the condition has a considerable negative impact on QoL, irrespective of subtype. Approximately half of the participants in each cohort were dissatisfied with their facial appearance because of rosacea and felt unattractive because of it. Many participants in both cohorts reported worrying about how people react when they see the rosacea or were concerned about the possible misperceptions of others, possibly because they might think the participant is alcoholic, shy/blushing, unconfident, or unhealthy. Furthermore, multiple assessment instruments, including the IA-RFR, RosaQoL questionnaire, and SF-36 in both cohorts and the IA-RFB in the PPR cohort, pointed to rosacea having a substantial negative impact on participants in several aspects of QoL, including self-perception, emotional well-being, and functional limitations due to emotional problems.
While rosacea generally had a slightly greater negative impact on QoL in the PPR cohort than it did in the ETR cohort, specifically in domains of dissatisfaction with facial appearance, feeling unattractive, worrying about how other people react to rosacea, and perceptions related to their success, confidence, shyness, or health, the burden of disease in ETR participants was also important. Most participants in the current study with ETR and PPR had mild or moderate rosacea, which correlates with RosaQoL severity scores of “very good” or “good” in the validation study for this instrument described by Nicholson et al.18 Those authors demonstrated that there was a roughly linear relationship between the severity of rosacea and scores on the three main domains of the RosaQoL questionnaire, suggesting that QoL was worse for participants with severity scores of very good or good compared with participants with severity scores of excellent, so that even mild rosacea could be associated with an important impact on QoL.18 Others have demonstrated that clinical improvement in disease severity is associated with improved QoL as measured by changes in RosaQoL scores.20 Thus, the goal of treatment for patients with moderate-to-severe rosacea should be the safe, effective improvement of clinical symptoms, as well as improvements in QoL.
The primary symptom of facial erythema had a negative effect on individuals in the ETR and PPR cohorts for all domains of the IA-RFR. Interestingly, for the PPR cohort, the data from the IA-RFR and IA-RFB suggested that facial erythema had a greater negative impact on the overall score and the Self-perception and Grooming domains than did facial bumps and pimples, whereas bumps and pimples had a greater negative impact on the Emotional and Social Domains.
This study also indicates that rosacea has broad negative impact on patient well-being in both physical and emotional domains. SF-36 is a general, validated QoL instrument that not only allows assessment of the physical and emotional impact of a disease state but also allows comparison with other diseases and within population norms for healthy individuals.21 Findings from the SF-36 showed that the ETR and PPR cohorts achieved poorer scores than the general US population on multiple domains. With most researchers indicating that a difference of 5 to 10 points is clinically significant,21 only scores in the Energy/Fatigue domain approached clinical significance for the ETR cohort compared with the general population.19 For PPR, scores in the Role Limitations Due to Emotional Problems, Emotional Well-being, Social Functioning, and Energy/Fatigue domains appeared to be clinically significant for the PPR cohort compared with the general population. The mean BMI in our population was slightly higher than the mean BMI reported for the general population in the 2009–2010 National Health and Nutrition Examination Survey,22 with 69.0 percent classified as overweight or obese.22 Since BMI was not controlled for in this analysis, it is possible that the higher BMI could account for some of the SF-36 results. However, given the increasing rate of overweight and obesity in the US, it is also possible that the population in this study, which was conducted in 2015, is representative of the current population.
A recent systematic review reported on 12 observational and prospective studies investigating different aspects of QoL in participants with various subtypes of rosacea, each utilizing validated health-related QoL instruments.7 While most studies enrolled fewer than 200 participants, enrollment in one-third of the studies ranged from 308 to 966 participants. All of the studies reported substantial negative effects of rosacea on the health-related QoL of the participants. In a separate survey of more than 400 individuals with rosacea conducted by the National Rosacea Society, rosacea was associated with substantial negative psychosocial effects, such as poor self-esteem, feeling embarrassed or frustrated, and feeling robbed of pleasure or happiness.23
The current findings from a large population in a cross-sectional study confirm those of earlier studies that indicated that rosacea is associated with negative psychosocial effects and decreased QoL.7,24 Prior studies have been limited to measurement of QoL with only one instrument, whereas the study reported here used multiple questionnaires evaluating different aspects of the psychosocial effects of rosacea.7 A separate publication from this survey describes findings regarding the most bothersome rosacea symptoms, treatment profiles, and expectations from treatment for participants with ETR and PPR. The majority of participants with ETR reported facial erythema, blushing, and/or flushing to be the most bothersome symptoms, while those with PPR also identified bumps and/or pimples as among the most bothersome symptoms. These results complement the current findings in that rosacea-associated facial erythema had a substantial negative impact on participants in both cohorts.
As described in the previous report from this survey, medication utilization was relatively low and satisfaction with both prescription and nonprescription agents by survey participants was low, with only about half of participants who used prescription agents being satisfied or very satisfied with treatment. Participants commonly reported relying on prescription agents to treat flare-ups rather than for continuous prophylactic use. Effective treatment for rosacea improves patients’ psychological symptoms and QoL related to rosacea.10,24,25 It might be helpful, therefore, for patients to be educated about the chronic nature of rosacea and the need for long-term treatment and to set reasonable expectations for treatment.24,26 This might in turn lead to greater satisfaction with treatment and associated improvements in psychosocial symptoms and QoL.
This study obtained a wide range of data from a single large cohort of participants with self-reported ETR and PPR. In addition, multiple survey instruments were used to assess the impact of rosacea from a variety of perspectives in this population. Questionnaires on coping and avoidance were modeled after the SWAP questionnaire, which was validated for use by burn patients, and the modified SWAP questionnaire, which was adapted and validated for use by patients with systemic sclerosis,13,14 and examined attitudes, beliefs, self-perceptions, and satisfaction with appearance as a result of having rosacea. Rosacea-specific instruments, including the validated RosaQoL questionnaire18 and the
IA-RFR, addressed rosacea impact on QoL based on specific features of rosacea.
Limitations. Limitations of this Internet-based survey include aspects of the electronic data collection methodology that could allow for selection bias, the reliance on self-reported disease diagnosis from participants and clinical history rather than on reports from medical professionals, and the relatively low recruitment of individuals with severe ETR and PPR. However, the last issue might be of limited importance when considering the psychosocial effects of rosacea, which do not always correlate with the severity of disease.27
Conclusion
Rosacea has wide-ranging negative effects on individuals who have a self-reported diagnosis of rosacea. These effects include impact on self-perceptions and emotional, social, and overall well-being, as well as rosacea-specific QoL, among individuals with ETR and PPR. Effective therapies that address the underlying etiology as well as the bothersome symptoms of rosacea, along with appropriate treatment education, are needed to achieve optimal aesthetic and psychosocial outcomes and improvements in QoL.
Acknowledgments
Writing and editorial assistance was provided to the authors by Michael L. Pucci, PhD, of Peloton Advantage, Parsippany, New Jersey, and was funded by Allergan plc, Dublin, Ireland.
References
- Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 1: a status report on the disease state, general measures, and adjunctive skin care. 2013;92(5):234–240.
- Baldwin HE. Diagnosis and treatment of rosacea: state of the art. J Drugs Dermatol. 2012;11(6): 725–730.
- National Rosacea Society site. Rosacea riddle now threatens more than 16 million Americans [press release]. 2010. Available at: http://www.rosacea.org/press/archive/20100401.php. Accessed: March 9, 2016.
- Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol. 2002;46(4):584–587.
- Del Rosso JQ, Gallo RL, Kircik L, Thiboutot D, Baldwin HE, Cohen D. Why is rosacea considered to be an inflammatory disorder? The primary role, clinical relevance, and therapeutic correlations of abnormal innate immune response in rosacea-prone skin. J Drugs Dermatol. 2012;11(6):694–700.
- National Rosacea Society site. Drake L. Survey shows rosacea’s emotional toll, positive effects of medical therapy. 2007. Available at: http://www.rosacea.org/rr/2007/spring/article_3.php. Accessed: March 9, 2016.
- van der Linden MM, van Rappard DC, Daams JG, et al. Health-related quality of life in patients with cutaneous rosacea: a systematic review. Acta Derm Venereol. 2015;95(4):395–400.
- Beikert FC, Langenbruch AK, Radtke MA, Augustin M. Willingness to pay and quality of life in patients with rosacea. J Eur Acad Dermatol Venereol. 2013;27(6):
734–738. - Aksoy B, Altaykan-Hapa A, Egemen D, Karagoz F, Atakan N. The impact of rosacea on quality of life: effects of demographic and clinical characteristics and various treatment modalities. Br J Dermatol. 2010;163(4):
719–725. - Moustafa F, Lewallen RS, Feldman SR. The psychological impact of rosacea and the influence of current management options. J Am Acad Dermatol. 2014;71(5):973–980.
- Li J, Li M, Chen Q, et al. Quality of life among patients with rosacea: an investigation of patients in China using two structured questionnaires. J Eur Acad Dermatol Venereol. 2016;30(10):e98–e99.
- Del Rosso JQ, Tanghetti EA, Baldwin HE, Rodriguez DA, Ferrusi IL. The burden of illness of erythematotelangiectatic rosacea and papulopustular rosacea: findings from a web-based survey. J Clin Aesthet Dermatol. 2017 June 1 [epub ahead of print].
- Lawrence JW, Heinberg LJ, Roca R, et al. Development and validation of the satisfaction with appearance scale: assessing body image among burn-injured patients. Psychol Assess. 1998;10(1):64–70.
- Heinberg LJ, Kudel I, White B, et al. Assessing body image in patients with systemic sclerosis (scleroderma): validation of the adapted Satisfaction with Appearance Scale. Body Image. 2007;4(1): 79–86.
- Ferrusi IL, Ahluwalia G, Andrae DA. Development and validation of the impact assessment for rosacea facial redness (IA-RFR) [poster]. Presented at: Annual Meeting of the International Society for Pharmacoeconomics and Outcomes Research; May 20–24, 2017; Boston, MA.
- Chren MM, Lasek RJ, Quinn LM, et al. Skindex, a quality-of-life measure for patients with skin disease: reliability, validity, and responsiveness. J Invest Dermatol. 1996;107(5):707–713.
- Chren MM, Lasek RJ, Flocke SA, Zyzanski SJ. Improved discriminative and evaluative capability of a refined version of Skindex, a quality-of-life instrument for patients with skin diseases. Arch Dermatol. 1997;133(11):1433–1440.
- Nicholson K, Abramova L, Chren MM, et al. A pilot quality-of-life instrument for acne rosacea. J Am Acad Dermatol. 2007;57(2):213–221.
- McDowell I. The Short-form-36 Health Survey: Measuring Health: A Guide to Rating Scales and Questionnares. 3rd ed. New York, NY: Oxford University Press; 2006:
649–665. - Baldwin HE. A community-based study of the effectiveness of doxycycline 40 mg (30-mg immediate-release and 10-mg delayed-release beads) on quality of life and satisfaction with treatment in participants with rosacea. 2010;86(5 Suppl):26–36.
- Obidoa CA, Reisine SL, Cherniack M. How does the SF-36 perform in healthy populations? A structured review of longitudinal studies. J Soc Behav Health Sci. 2010;4(1):30–48.
- Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. 2012;307(5):
491–497. - Coping with rosacea. 2016. Available at: http://www.rosacea.org/patients/materials/coping/managing.php#Managing. Accessed: March 29, 2016.
- Huynh TT. Burden of disease: the psychosocial impact of rosacea on a patient’s quality of life. Am Health Drug Benefits. 2013;6(6):348–354.
- Fleischer A, Suephy C. The face and mind evaluation study: an examination of the efficacy of rosacea treatment using physician ratings and patients’ self-reported quality of life. J Drugs Dermatol. 2005;4(5):585–590.
- Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 5: a guide on the management of rosacea. 2014;93(3):
134–138. - Bohm D, Schwanitz P, Stock GS, et al. Symptom severity and psychological sequelae in rosacea: results of a survey. Psychol Health Med. 2014;19(5):586–591.