
Moetaz El-Domyati, MD, Department of Dermatology, Al-Minya University, Al-Minya, Egypt; Tarek S. El-Ammawi, MD, Department of Dermatology, Al-Minya University, Al-Minya, Egypt; Walid Medhat, MD, Department of Dermatology, Al-Minya University, Al-Minya, Egypt, Department of Dermatology and Cutaneous Biology, Thomas Jefferson University, Philadelphia, Pennsylvania; Osama Moawad, MD, Moawad Skin Institute for Laser, Cairo, Egypt; My G. Mahoney, PhD, Department of Dermatology and Cutaneous Biology, Thomas Jefferson University, Philadelphia, Pennsylvania; Jouni Uitto, MD, PhD, Department of Dermatology and Cutaneous Biology, Thomas Jefferson University, Philadelphia, Pennsylvania
Disclosure: The authors report no relevant conflicts of interest. This work was in part supported by the Cultural and Educational Bureau of the Republic of Egypt to Dr. Medhat and by NIH grant R01 AR28450 to Dr. Uitto.
Abstract
Objectives: Electro-optical synergy technology is one of the most recently described methods for nonablative skin rejuvenation. The aim of this study is to evaluate the effects of electro-optical synergy on connective tissue composition by histological and immunohistochemical techniques coupled with computerized morphometric analysis. Design: A prospective clinical study. Participants: Six volunteers with Fitzpatrick skin types 3 to 4 and Glogau class I to II wrinkles were subjected to three months (6 sessions at 2-week intervals) of electro-optical synergy treatment. Measurements: Standard photographs and skin biopsies were obtained at baseline as well as three and six months after the start of treatment. The authors performed quantitative evaluation of total elastin, tropoelastin, collagen types I, III, and VII, and newly synthesized collagen. Results: Noticeable clinical and histological improvement was observed after electro-optical synergy treatment. A statistically significant increase in the means of collagen types I, III, and VII, as well as newly synthesized collagen, together with increased levels of tropoelastin, were detected, while the mean level of total elastin was significantly decreased at the end of treatment and three months post-treatment. Conclusion: Electro-optical synergy is an effective treatment for contouring facial skin laxity. This modality stimulates the repair processes and reverses the clinical, as well as the histopathological, signs of aging with the advantage of being a relatively risk-free procedure with minimal patient recovery time. (J Clin Aesthet Dermatol. 2010;3(12):22–30.)
Photoaging was first described in 1986 as the consequence of chronic exposure to the elements, primarily ultraviolet (UV) radiation, on the skin.[1,2] Clinically, photoaged skin is characterized by wrinkles, roughness, laxity, increased fragility, pigmentary changes, telangiectasia, and delayed wound healing.[3] The histological and ultrastructural hallmark of photodamaged skin is the accumulation of elastotic material in the papillary and mid dermis, a process known as solar elastosis.[4] This is accompanied by quantitative changes in collagen biosynthesis, which are reflected by a steady decline in collagen content by approximately one percent per year.[4,5] The collagen fiber architecture becomes disorganized, with enhanced breakdown and reduced network formation.[6] These alterations contribute to the sagging and wrinkling of the skin.[7] Previous data showed an increased interest in nonablative treatments for skin aging, which are used to rejuvenate the skin ‘‘safely and effectively,’’ with little or no down time and fewer complications than observed with ablative treatments.[7] Intense pulsed light (IPL) and radiofrequency (RF) are two examples of effective nonablative treatments of skin aging. Recently, the combination of both energies in the same pulse profile to produce electro-optical synergy (ELOS) has been used to improve textural changes and rejuvenation of photoaged skin.[8] The mechanism of this novel technology is based on the following two combined approaches: a) the light-based technology IPL, a photothermal mechanism, where the pulsed optical energy targets and preheats distinct chromophores, producing differences in temperature between the target and the surrounding tissue[9] and b) RF, the creation of stress waves at the skin surface, producing uniform heat at a controlled depth in the dermal layers. Thus, both energies create a thermal wound at the targeted area, with subsequent remodeling and reorientation of collagen fibers and the formation of new collagen, which is achieved after months of treatment.[10,11] The purpose of the present study was to objectively quantify the histological changes in the skin and to evaluate the corresponding clinical outcome after the use of the ELOS approach as a nonablative treatment for skin rejuvenation.
Materials and Methods
Protocol of treatment. The present study was conducted on six volunteers, four males and two females, with Fitzpatrick skin type 3 to 4 and Glogau class I to II wrinkles,[12] who were attending the dermatology outpatient clinic at Al-Minya University Hospital, Al-Minya, Egypt. Their ages ranged from 41 to 69 years, with an average of 57±11.8. Treatment and study details were fully explained to the subjects and all signed informed consent forms. The clinicians marked the periorbital area on both sides (treatment area) and applied a topical anesthetic cream (lidocaine 2.5% + prilocaine 2.5%) as a thick coating, which was left under occlusion for 90 minutes. The cream was then gently removed, and the subject was positioned for treatment. A conductive cooling gel was applied to the treatment site to ensure uniform energy conduction and enhance the thermal and electrical contact between the hand piece and the skin.
A continuous external air cooling system was used throughout the treatment session. The authors used an E light device (Beijing ADSS Development Co, Beijing, China), which produces a combination of IPL and RF energies in the same pulse profile, with the following specifications: 12x30mm spot size hand piece, 640nm cut-off filter, 25J/cm2 energy, 30ms pulse duration, and 30W RF power. Each volunteer received 12 pulses per side (a total of 24 pulses); intolerable heat sensation was not reported during these sessions. Volunteers were subjected to a total of three months of treatment (6 sessions at 2-week intervals). They were instructed to avoid sun exposure and use a prescribed sunscreen. In addition, the use of ice packs after each session was avoided to promote a healing response. Photographs were taken before and at the end of treatment, as well as at three months post-treatment. At these time points, punch biopsies (3mm) were obtained from facial skin. Biopsies after treatment were taken from a site near the pretreatment ones. Tissues were fixed in 10% buffered formalin, embedded in paraffin, and sectioned into 5µm-thick sections.
Histology and immunostaining. All histological and immunostaining analyses were carried out in the Department of Dermatology and Cutaneous Biology, Thomas Jefferson University, Philadelphia, Pennsylvania. Histopathological studies were performed using standard hematoxylin and eosin (H&E), Verhoeff van Gieson (HT25A; Sigma Aldrich, St. Louis, Missouri) and picrosirius red staining (Direct Red 80, Sigma Aldrich). The authors performed immunoperoxidase staining for total elastin and collagen types I and III. Briefly, tissue slides were heated at 60ºC for 30 to 60 minutes and then deparaffinized and antigens retrieved in 0.1M sodium citrate (pH 6.0) for five minutes by the microwave method. Nonspecific sites were blocked in blocking buffer (5% normal goat serum, 1% BSA and 0.02% TX-100 in PBS), and tissues were incubated with antibodies to elastin (1:300; E4013; Sigma Aldrich), type I collagen (1:400; sc-59772; Santa Cruz Biotech, California), and type III collagen (1:600; ab6310; Abcam, Cambridge, Massachusetts). Samples were then incubated with biotinylated secondary antibody (1:200; PK-6102; Vector Labs, California), ABC reagent (Vectastain Elite ABC Peroxidase Kits Mouse; PK-6102; Vector Labs), and stained with DAB Chromogen Substrate Kit (K3468; Dako, California). All slides were counterstained with hematoxylin (7211; Thermo Scientific, Iowa) and mounted for viewing.
Indirect immunofluorescence (IF) was used for type VII collagen and tropoelastin. After deparaffinization and antigen retrieval as described above, tissue slides were incubated with antibodies to type VII collagen (1:600; sc-33710; Santa Cruz Biotech), secondary antibody Alexa Fluor goat anti-mouse immunoglobulin (IgG) 594 (1:400; Molecular Probes, Eugene, OR), and 4’,6-Diamidino-2-phenylindole dihydrochloride (DAPI) (1:1000; D8417; Sigma Aldrich) for nuclear staining, and slides were then mounted for viewing. For tropoelastin, the authors used the microprobe system (Fisher Scientific #FD-188-10A) with reagents from Open Biosystems (Huntsville, Alabama) as previously described.[13]
Tissues were incubated with blocking buffer (5% normal goat serum, 1% BSA and 0.01% Triton-X-100 in PBS), tropoelastin antibody GA317 (1:400; Elastin Products, Owensville, Missouri), and Alexa Fluor goat anti-rabbit IgG 594 secondary antibody (1:400; Molecular Probes). All histometric evaluations were carried out using computer-based software (Image-Pro Plus; Media Cybernetics, Silver Spring, Maryland).
Statistical analysis. Quantitative evaluations of histological measurements were analyzed using the Software Package for Statistical Science (SPSS) (SPSS for Windows; Version 16, SPSS Inc.; Chicago, Illinois). Statistical analysis was performed using One-way ANOVA, Wilcoxon-matched pairs signed ranks, and Chi-square tests. Data were expressed as mean value ± standard deviation (SD). Statistical significance was defined as p?0.05.
Results
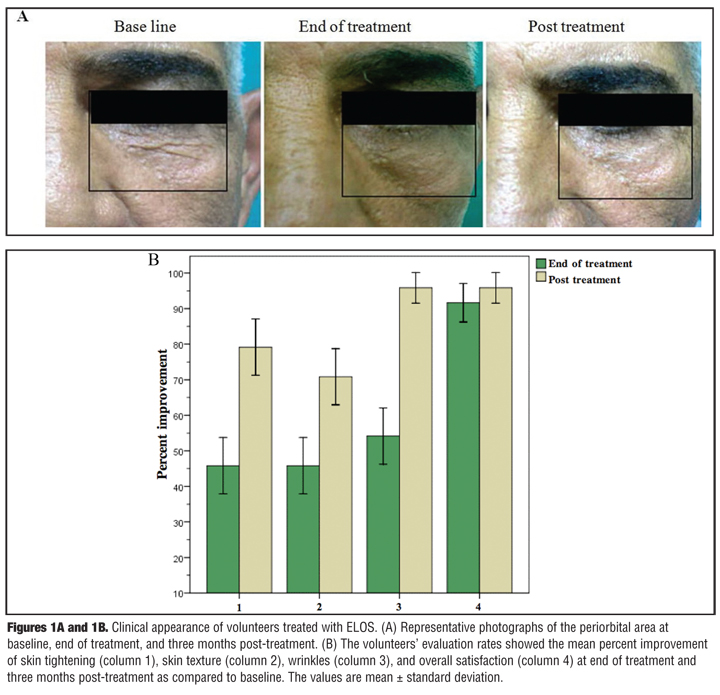
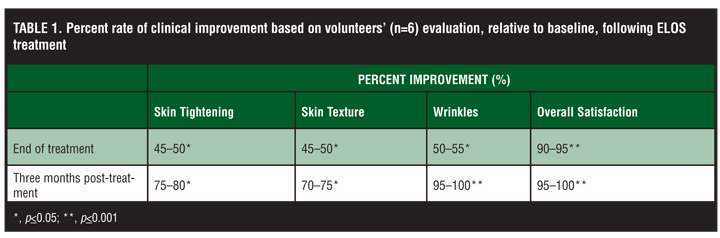
Clinical assessment. All participants completed the ELOS study and showed both subjective and objective improvement in the clinical appearance of wrinkles in the periorbital region (Figure 1A). At each endpoint (before, at the end, and three months after treatment), the volunteers, two dermatologists, and two independent observers were asked to evaluate the following criteria: wrinkle improvement, skin tightening and texture, and overall satisfaction. Their evaluation was assessed on a five-point scale (none=0%, mild=1%–25%, moderate=26%–50%, good=51%–75%, and very good=76%–100%). The results were tabulated and compared to baseline for statistical significance with the Pearson Chi-square test (Table 1 and Figure 1B). The dermatologists and the independent observers’ assessments were comparable to the volunteers’ evaluation rates. In addition, potential side effects, including erythema, edema, and hypo- or hyperpigmentation, were evaluated on a four-point scale (none, mild, moderate, and severe); none of the subjects experienced any complications.
{kind=link}
{kind=link}
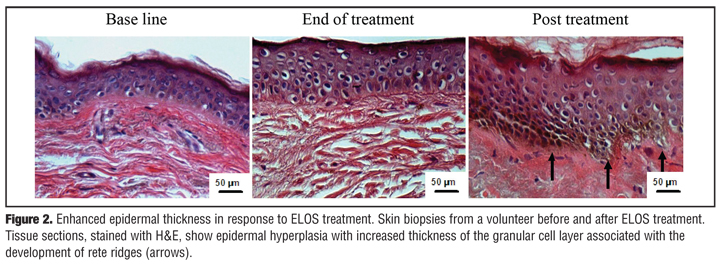
Histological evaluation of the epidermis. Microscopic examination of H&E stained sections at the end of treatment showed, as compared to the baseline, a significant increase in the mean of epidermal thickness from 58.5±3.4µm to 75.8±5.1µm (p?0.001), which continued to increase three months post-treatment to 82.8±3.6µm (p?0.001) Figure 2). This was associated with overall morphological and architectural improvements of the epidermis, with marked undulations of the dermo-epidermal junction. There was an increase in the number and size of the cells in the granular layer, which was reflected as a significant increase in granular layer thickness from 5.9±1.2µm before treatment to 14.3±1.6µm (p?0.0001) at the end of treatment and 20.6±2.9µm three months post-treatment (p?0.0001).
{kind=link}
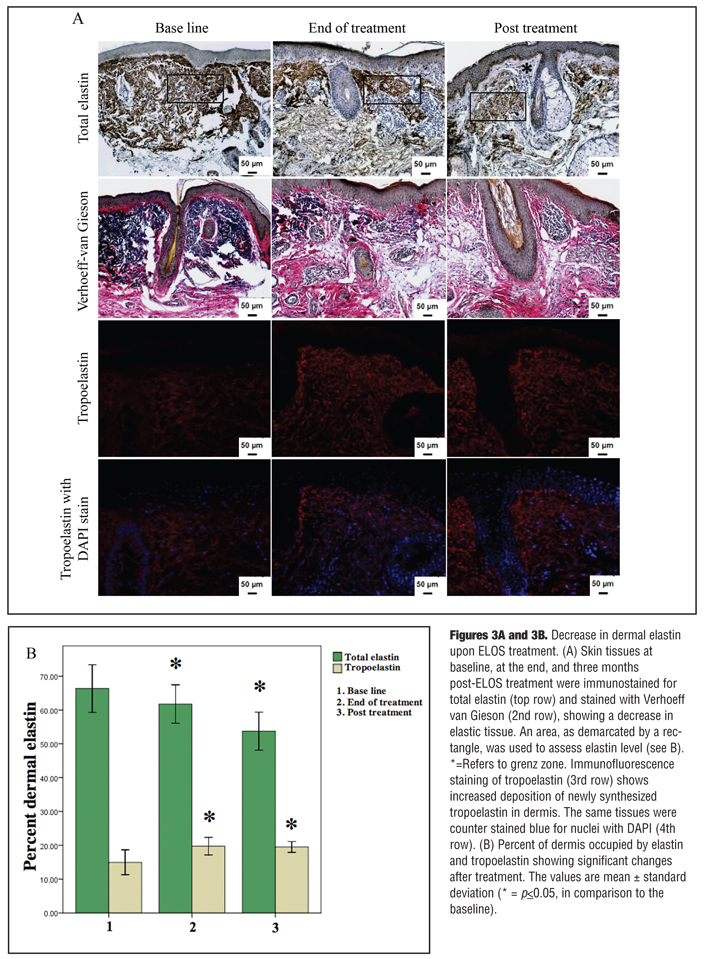
Evaluation of changes in the elastic structures in the dermis. Through different decades of life, quantitative as well as qualitative changes in the elastic and collagen fibers are observed. Dermal elastosis, which largely consists of a gradual accumulation of thickened, tangled, and ultimately granular amorphous and pleiomorphic elastic structures, is noticeable in the papillary and mid-dermis.[2] The authors examined the effects of ELOS treatment on total dermal elastin structures by measuring the percent area of dermis occupied by immunohistochemically detectable elastin. They observed a statistically significant decrease in elastin staining from 66.3±6.9 percent at baseline to 61.7±3.2 percent after ELOS treatment (p?0.002); total elastin continued to decrease three months after treatment (53.7±5.4%; p?0.005) (Figure 3). The decline in elastin content was associated with a translocation of the solar elastotic material away from the epidermis, accompanied by the restoration of normal-appearing elastic fibers within the papillary and upper reticular dermis. The authors also used the Verhoeff van Gieson special stain (Figure 3A) to differentiate the elastic tissues (blue-black to black), which are decreased in content after treatment, from the collagen fibers (red).
{kind=link}
Elastic fibers are composed mainly of elastin, a connective tissue protein which is initially synthesized as tropoelastin.[13] Thus, the authors evaluated the rate of elastin biosynthesis by quantifying newly synthesized tropoelastin. Compared to the baseline, the results showed a significant increase in the mean of tropoelastin from 14.9±3.5 percent to 19.7±2.4 percent at the end of treatment, and 19.5±1.5 percent three months post-treatment (p?0.021 and 0.026, respectively) (Figure 3).
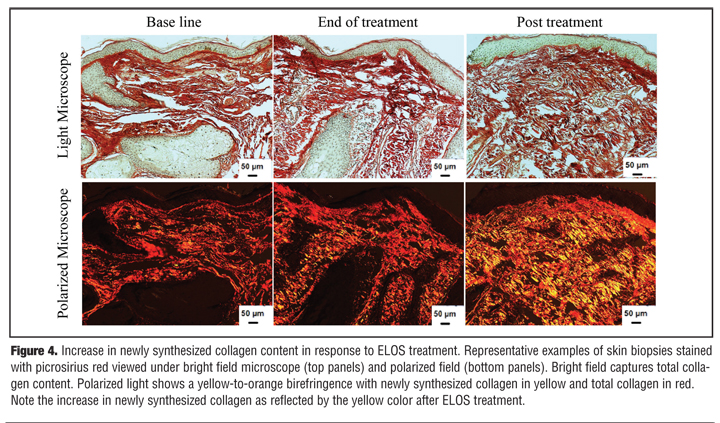
Quantitation of collagen content in the dermis. Mature collagen fibers change color under polarized light (birefringence) with a subsequent decrease in light penetration. When tissues are stained with picrosirius red and viewed under a polarized microscope, large collagen fibers stain red while the thinner ones, which represent the newly synthesized fibers, are stained yellow to orange.[14,15] Here, the authors show an increase in newly synthesized collagen fibers, as reflected by the presence of yellow-orange birefringence, from 17.9±4.4 percent at the baseline to 23.9±3.1 percent (p?0.021) at the end of ELOS treatment, and 27.9±2.8 percent (p?0.001) at three months post-treatment (Figure 4). In summary, the data show that enhanced collagen expression and new collagen formation continued to increase three months after cessation of treatment.
{kind=link}
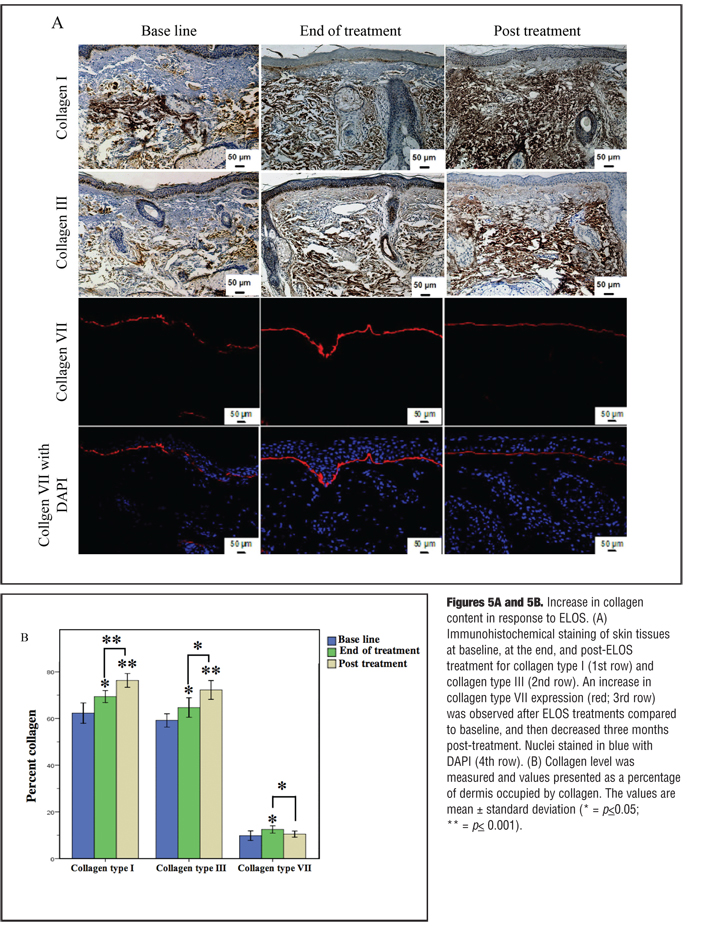
Immunohistochemical staining for total collagen also revealed a narrow collagen band, the grenz zone (6.3±1.1µm) at the dermo-epidermal junction before treatment, which is significantly increased to 11.8±2.4µm at the end of treatment (p?0.001), with a further increase in the thickness to 14.8±1.9µm (p?0.0001) at three months post-treatment. Quantitative evaluation of the percentage of dermis occupied by collagen showed a significant increase in the content of type I collagen (Figures 5A [1st row] and 5B in Figure 5) from 62.3±4.2% before treatment to 69.4±2.4 percent at the end of treatment (p?0.005), and 76.3±2.8 percent three months post-treatment (p?0.0001). Also, an assessment of collagen type III revealed a significant increase from 59.2±2.7 percent at the baseline to 64.7±3.9 percent (p?0.019) at the end of treatment and 72.2±3.8 percent three months post-treatment (p?0.0001) (Figures 5A [2nd row] and 5B in Figure 5).
{kind=link}
Type VII collagen is the main component of the anchoring fibrils mediating dermal-epidermal adherence in human skin.[16] The effect of the aging process on collagen VII biosynthesis and degradation has been previously noted,[17–19] so the authors quantified the level of collagen VII expression in response to ELOS treatment. The data revealed a significant increase in type VII collagen expression from 9.8±1.9 percent before treatment to 12.5±1.5 percent at the end of treatment (p?0.025), which was followed by a return to slightly above the pretreatment level (10.5±1.2%) at three months post-treatment (p?0.031) compared to the end of treatment (Figures 5A [3rd and 4th rows] and 5B in Figure 5).
Discussion
Various methods, including topical preparations, dermabrasion, and chemical peeling, have been used to promote normalization of actinically damaged skin.[20] More recently, laser skin rejuvenation has emerged as an effective aesthetic treatment.[21] Nonablative photo rejuvenation has become an integral modality to reverse the signs of photoaged skin, as it enhances dermal remodeling with little down time and few complications.[22] A major concern with nonablative skin rejuvenation studies is that few standardized and objective approaches have been used to measure the depth of wrinkles, as well as the elasticity of skin. Additionally, the clinical results are often dependent on the subjective estimate by physicians and/or volunteers.[23–25] ELOS was recently introduced as a new nonablative treatment for skin rejuvenation and thus very little is known of its efficacy or its effects on skin biology.[26–28] In this study, the authors assessed the effects of ELOS treatment on skin tightening, appearance, and structural composition in photodamaged skin in individuals 41 to 69 years of age. Clinical evaluation of volunteers showed a noticeable improvement in periorbital wrinkles, skin tightening, and texture at the end of treatment, with continued improvement three months post-treatment. These findings are in agreement with Sadick et al,[26] who reported a noticeable improvement in aged skin using an ELOS system; the overall skin improvement as compared to the baseline was rated at 75.3 percent, and the overall average wrinkle improvement was 41.2 percent. Improvement in skin laxity was rated at 62.9 percent. Skin texture was reported to improve 74.1 percent, and overall patient satisfaction was 92 percent after 15 weeks of treatment. Hammes et al[28] stated that multiple treatments with the ELOS system produced objective, as well as subjective, improvement of periorbital and perioral wrinkles.
The in-vivo response to thermal wound healing consists of three consecutive stages: inflammatory, proliferative, and remodeling.[3] This might explain why clinically visible results were only achieved between 3 and 6 months after the beginning of treatment. Photoaged skin is associated with a decrease in epidermal thickness, with flattening of the rete ridges.[29] Although both RF and IPL energies target the dermal layer of the skin, in this study, the authors observed striking changes in histological features of the epidermis. They showed a noticeable increase in epidermal thickness at the end of treatment, which continued to increase three months post-treatment. These findings suggest that the proliferating epidermis may contribute to the improvement of skin appearance; however, further in-depth studies are necessary.
Microscopic changes associated with wrinkles occur primarily in the dermis. In sun-damaged skin, the main dermal alteration is the deposition of large clumps of abnormal elastotic material replacing the normally collagen-rich dermis.[30] In this study, the authors evaluated the effects of ELOS treatment on total elastin deposition, as it is one of the major changes occurring in aged skin. The results showed a significant decrease in total elastin content at the end of treatment, which continued to decrease three months post-treatment. This decrease was accompanied by the downward translocation of the elastotic material with reorientation of the elastic fibers. In photoaged skin, there is an ongoing proteolytic degradation of normal elastic fibers, combined with distinctly decreased normal elastin biosynthesis.[13] Accordingly, the authors assessed the changes in the level of tropoelastin, the precursor of elastin biosynthesis. The results showed a significant increase in the levels of tropoelastin at the end of treatment, which remained high three months post-treatment (Figure 3A in Figure 3). These findings suggest that ELOS may activate dermal fibroblasts to produce new elastin.
Repeated thermal wound healing stimulates fibroblasts to enhance new collagen deposition and remodeling, resulting in further collagen tightening and an overall increase in collagen content.[31] In this study, the authors showed a significant increase in the thickness of the narrow collagen band, the grenz zone, present at the dermo-epidermal junction, at the end of treatment, as well as post-treatment, which may explain why the elastotic material was translocated downward away from the epidermis as a response to ELOS treatment. Wrinkle reduction, by means of thermal heat applied to the dermis, is also based on the stimulation of new collagen formation. In this study, quantitative evaluation of dermal collagen revealed a significant increase in types I, III, and VII collagens at the end of ELOS treatment. Three months post-treatment, the increase in types I and III collagens continued while type VII collagen was significantly decreased close to the pretreatment level. Previous studies showed that both fibroblasts and keratinocytes synthesize type VII collagen,[16] which could possibly explain the decrease in collagen VII levels three months post-treatment, as the keratinocytes might stop expressing this protein after the cessation of ELOS treatment. However, further studies are needed to resolve this question. Although others have shown that ELOS can improve skin appearance,[8,26,28,32] this study provided an in-depth analysis of the histological skin changes after this treatment modality.
To the best of the authors’ knowledge, no previous work concerning quantitative changes of newly formed collagen (using picrosirius red stain); collagen types I, III, and VII; and elastin and tropoelastin (using immunohistochemistry) were reported after ELOS treatment of photoaging.
In conclusion, ELOS is an effective and promising procedure that can be used to rejuvenate aged skin and reverse the signs of photoaging safely and effectively. This modality stimulates the remodeling process and improves the clinical and histological signs of aging with the advantage of being a safe procedure and avoiding significant down time. The authors are aware that one of the limitations of the study is the relatively small number of volunteers. However, the results showed statistically significant evidence of clinical and histological improvement in response to ELOS treatment.
Acknowledgment
The authors thank Carol Kelly and Alicia Dowling for their help in the preparation of this article. They also thank Shayna Ravindran and Joyce Tsai for technical assistance.
References
1. Kligman LH, Kligman AM. The nature of photoaging: its prevention and repair. Photodermatol. 1986;3:215–227.
2. El-Domyati M, Attia S, Saleh F, et al. Intrinsic aging vs. photoaging: a comparative histopathological, immuno-histochemical, and ultrastructural study of skin. Exp Dermatol. 2002;11:398–405.
3. Helfrich YR, Sachs DL, Voorhees JJ. Overview of skin aging and photoaging. Dermatol Nurs. 2008;20:177–183.
4. Uitto J. The role of elastin and collagen in cutaneous aging: intrinsic aging versus photoexposure. J Drugs Dermatol. 2008;7:S12–S16.
5. Sadick NS, Weiss R. Intense pulsed-light photorejuvenation. Semin Cutan Med Surg. 2002;21:280–287.
6. El-Domyati M, Attia S, Saleh F, et al. Effect of topical tretinoin on photoaged facial skin: a histometric, immunohistochemical and ultrastructural study. J Cosmet Dermatol. 2004;3: 191–201.
7. Kim KH, Geronemus RG. Nonablative laser and light therapies for skin rejuvenation. Arch Facial Plast Surg. 2004;6:398–409.
8. Sadick NS, Makino Y. Selective electro-thermolysis in aesthetic medicine: a review. Lasers Surg Med. 2004;34: 91–97.
9. Trelles MA, Allones I, Velez M. Nonablative facial skin photorejuvenation with an intense pulsed light system and adjunctive epidermal care. Lasers Med Sci. 2003;18:104–111.
10. Bogle MA, Ubelhoer N, Weiss RA, et al. Evaluation of the multiple pass, low fluence algorithm for radiofrequency tightening of the lower face. Lasers Surg Med. 2007;39: 210–217.
11. Kist D, Burns AJ, Sanner R, et al. Ultrastructural evaluation of multiple pass low energy versus single pass high energy radio-frequency treatment. Lasers Surg Med. 2006;38:150–154.
12. Glogau RG, Matarasso SL. Chemical peels. Trichloroacetic acid and phenol. Dermatol Clin. 1995;13:263–276.
13. Mahoney MG, Brennan D, Starcher B, et al. Extracellular matrix in cutaneous aging: the effects of 0.1% copper-zinc malonate-containing cream on elastin biosynthesis. Exp Dermatol. 2009;18:205–211.
14. Whittaker P, Kloner RA, Boughner DR, et al. Quantitative assessment of myocardial collagen with picrosirius red staining and circularly polarized light. Basic Res Cardiol. 1994;89:397–410.
15. Rich L, Whittaker P. Collagen and picrosirius red staining: a polarized light assessment of fibrillar hue and spatial distribution. Braz J Morphol Sci. 2005;22:97–104.
16. Chung HJ, Uitto J. Type VII collagen: the anchoring fibril protein at fault in dystrophic epidermolysis bullosa. Dermatol Clin. 2010;28:93–105.
17. Watson RE, Ball SG, Craven NM, et al. Distribution and expression of type VI collagen in photoaged skin. Br J Dermatol. 2001;144:751–759.
18. Villone D, Fritsch A, Koch M, et al. Supramolecular interactions in the dermo-epidermal junction zone: anchoring fibril-collagen VII tightly binds to banded collagen fibrils. J Biol Chem. 2008;283:206–213.
19. Amano S. Possible involvement of basement membrane damage in skin photoaging. J Investig Dermatol Symp Proc. 2009;14:2–7.
20. Mezzana P, Valeriani M. Rejuvenation of the aging faces using fractional photothermolysis and intense pulsed light: a new technique. Acta Chir Plast. 2007;29:47–50.
21. Nelson JS, Majaron B, Kelly KM. What is nonablative photorejuvenation of human skin? Semin Cutan Med Surg. 2002;21:238–250.
22. DeHoratius DM, Dover JS. Nonablative tissue remodeling and photorejuvenation. Clin Dermatol. 2007;25:474–479.
23. Goldberg DJ, Rogachefsky AS, Silapunt S. Non-ablative laser treatment of facial rhytides. A comparison of 1450 nm diode laser treatment with dynamic cooling device as opposed to treatment with dynamic cooling alone. Lasers Surg Med. 2002;30:79–81.
24. Fournier N, Dahan S, Barneon G, et al. Nonablative remodeling: clinical, histologic, ultrasound imaging, and profilometric evaluation of a 1540nm Er:glass laser. Dermatol Surg. 2001;27:799–806.
25. Grema H, Greve B , Raulin C. Facial rhytides—subsurfacing or resurfacing? A review. Lasers Surg Med. 2003;32: 405–412.
26. Sadick NS, Alexiades-Armenakas M, Bitter PJ, et al. Enhanced full-face skin rejuvenation using synchronous intense pulsed optical and conducted bipolar radiofrequency energy (ELOS): introducing selective radiophotothermolysis. J Drugs Dermatol. 2005;4:181–186.
27. Bitter PJ, Stephen Mulholland R. Report of a new technique for enhanced non-invasive skin rejuvenation using a dual mode pulsed light and radio-frequency energy source: selective radio-thermolysis. J Cosmet Dermatol. 2002;1: 142–143.
28. Hammes S, Greve B, Raulin C. Electro-optical synergy (ELOS) technology for non-ablative skin rejuvenation: a preliminary prospective study. J Eur Acad Dermatol Venereol. 2006;20:1070–1075.
29. Ruiz-Esparza J, Gomez JB. Nonablative radiofrequency for active acne vulgaris: the use of deep dermal heat in the treatment of moderate-to-severe active acne vulgaris (thermotherapy): a report of 22 patients. Dermatol Surg. 2003;29:333–339.
30. El-Domyati M, Attia S, Saleh F, et al. Trichloroacetic acid peeling versus dermabrasion: a histometric, immunohistochemical, and ultrastructural comparison. Dermatol Surg. 2004;30:179–188.
31. Ruiz-Esparza J. Nonablative radiofrequency for facial and neck rejuvenation. A faster, safer, and less painful procedure based on concentrating the heat in key areas: the ThermaLift concept. J Cosmet Dermatol. 2006;5:68–75.
32. Doshi SN, Alster TS. Combination radiofrequency and diode laser for treatment of facial rhytides and skin laxity. J Cosmet Laser Ther. 2005;7:11–15.