
by Sanjay Bhambri, DO; Chief Resident, Dermatology, Valley Hospital Medical Center, Las Vegas, Nevada;
Avani Desai, MD, Dermatology Resident, SUNY Downstate Medical Center, Brooklyn, New York;
James Q. Del Rosso, DO, FAOCD, Clinical Associate Professor (Dermatology), University of Nevada School of Medicine and Touro University College of Osteopathic Medicine; Dermatology Residency Director, Valley Hospital Medical Center and Las Vegas Skin and Cancer Clinics, Las Vegas and Henderson, Nevada;
Narciss Mobini, MD, Clinical Assistant Professor, Department of Pathology, Dermatology, and Medicine, University of Nevada School of Medicine, Las Vegas, Nevada
Abstract
Dermatofibrosarcoma protuberans (DFSP) is a rare, slow-growing fibrohistiocytic neoplasm that commonly favors young to middle-aged adults. It is most commonly seen on the trunk and frequently recurs locally after an incomplete excision, but distant metastasis is rare. Mohs micrographic surgery (MMS) is the treatment of choice for DFSP.
(J Clin Aesthetic Derm. 2008;1(1):34–36)
*******************************************************************************************************************************************************
Dermatofibrosarcoma protuberans (DFSP) is a rare, slow-growing, fibrohistiocytic neoplasm with intermediate- to low-grade malignancy that commonly favors young to middle-aged adults. It is most commonly seen on the trunk followed by the proximal extremities and the head and neck.[1] The potential for distant metastasis is low, but DFSP frequently recurs locally after incomplete excision. The general immunostaining pattern of DFSP is CD34 positive and factor XIIIa negative. Mohs micrographic surgery (MMS) is the treatment of choice for DFSP.
Case Report
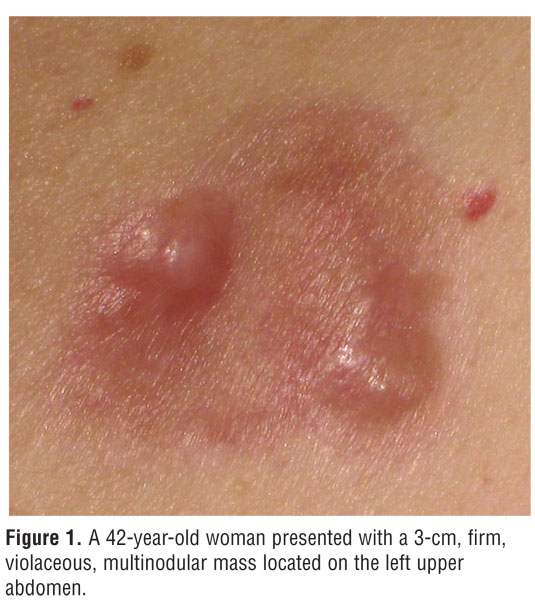
A 42-year-old woman presented to our office with a 3-cm, firm, violaceous, multinodular mass located on the left upper abdomen (Figure 1). The lesion had been present for approximately five years and was progressively increasing in size. She complained of tenderness upon palpation of the lesion. She denied any treatment of the lesion in the past. No other lesion was noted. She denied any recent weight loss, night sweats, fevers, or chills. The lymph nodes in the head and neck region and the axillae were nonpalpable.
{kind=link}
The biopsy showed a spindle-cell neoplasm located primarily in the dermis with infiltration of the subcutaneous fat in a lace-like pattern. The neoplastic cells showed uniform slender and elongated nuclei with scanty pale cytoplasm. The spindle cells were arranged as intersecting fascicles and as whorls in a storiform pattern. The biopsy findings were consistent with the diagnosis of DFSP. The constituent cells reacted positively with CD34 immunostain and were negative for factor XIIIa.
The patient decided to seek treatment from an oncologic surgeon out of state and was subsequently lost to follow-up.
Discussion
DFSP is a low-grade, relatively uncommon, soft-tissue sarcoma that was originally described in 1924 by Darier and Ferrand.[2,3] The term dermatofibrosarcoma protuberans was coined by Hoffman in 1925.[3] It accounts for less than five percent of soft-tissue tumors and 0.1 percent of all malignancies with an annual incidence of 0.8 to 4.5 per million.4,5 It is most commonly seen among those in their third or fourth decade and favors the trunk (40–60%), followed by the proximal extremities (20–30%) and the head and neck (10%–16%).[1,5] A slight male predominance has been reported among patients with DFSP.[6] It occurs less frequently in children, and congenital forms of DFSP have been reported in the literature.[7] The tumor has a low chance of metastasis, either to regional lymph nodes or distantly, but is aggressive locally. A local recurrence rate of DFSP of up to 60 percent has been reported.[8] The tumor most commonly presents as a slow-growing, asymptomatic, skin-colored, indurated, firm plaque that eventually develops violaceous to red-brown nodules that vary in size from one to several centimeters in diameter. DFSP may present as an atrophic plaque,[9] which may resemble morphea and can be misdiagnosed as such.
Pathogenesis
A genetic link has been found in some patients with DFSP, which frequently (more than 90 percent) exhibits translocation of chromosomes 17 and 22, t(17;22).[10,11] This rearrangement fuses the collagen, type I, alpha 1 (COL1A1) gene to the platelet-derived growth factor B-chain (PDGFB) gene. The resultant rearrangement causes unregulated expression of platelet-derived growth factor leading to constitutive activation of the platelet-derived growth factor receptor (PDGFR).[10,11] This step is believed to be a critical event in DFSP tumorigenesis. Germ-line mutations of p53 have been described in patients with DFSP and breast adenocarcinoma.[2] DFSP has been reported to develop after prolonged tanning-bed use.[12]
Histologic and immunohistochemical Features
The biopsy typically shows the lesion to be located primarily in the dermis with irregular infiltration of the subcutaneous fat in a lace-like pattern. The epidermis is usually spared, but can be hyperplastic. The lesion usually comprises fairly uniform spindle cells with elongated nuclei and scanty pale cytoplasm. Pleomorphism is minimal or absent. The cells are typically arranged in a storiform or a mat-like pattern. Immunohistochemically, in the plaque stage, the spindle-shaped cells are strongly positive for CD34 immunostaining.[13–15] Plaque and nodular areas are negative for factor XIIIa, which differentiates DFSP from a dermatofibroma.[14,15] The general immunostaining pattern of DFSP is thus CD34 positive and factor XIIIa negative. Dermatofibromas are CD34 negative and factor XIIIa positive.
DFSP is CD117 negative.[16,17] Cyclooxygenase-2 expression was not shown to be an effective diagnostic measure for distinguishing dermatofibroma from dermatofibrosarcoma protuberans.[18]
Management
MMS is the treatment of choice for DFSP. Prior to MMS, surgical excision with 3- to 5-cm-wide margins was the recommended treatment, but was associated with high rates of local recurrence. The extent of invasion is difficult to ascertain because of its ability to penetrate not only cutaneous and subcutaneous tissue, but also underlying fascia and muscle. In a three-dimensional view, the tumor can be visualized as sending projections in different directions so even a wide excision may leave residual tumor in a single or multiple foci.[19,20]
A recurrence rate of up to 20 percent with 3-cm surgical margins has been described.21 Ratner, et al., reported that a standard wide excision with a width of 1cm would leave residual tumor in 70.7 percent of tumors, a width of 2cm would leave residual tumor in 39.7 percent of tumors, a width of 3cm would leave residual tumor in 15.5 percent of tumors, and a width of 5cm would leave residual tumor in 5.2 percent of tumors. The authors concluded that MMS is the treatment of choice for DFSB.[19]
Nouri, et al., reported no recurrences in a series of 20 patients treated with MMS.8 The mean number of MMS stages done to achieve clear margins was 2.5. Snow, et al., reported no local recurrences and a five-year local cure rate of 100 percent in 29 patients who were treated with MMS.22 In the literature review conducted by Snow, et al., nine out of 136 patients treated with MMS developed local recurrences. Five patients developed recurrences even after undergoing the Mohs procedure twice. The local cure rates reported in that paper were 93.4 percent and 98.5 percent after first and second Mohs surgeries, respectively.[22] In the Geisinger experience, no local recurrences were seen in 35 patients at a mean follow-up of 39 months.[21]
Radiotherapy has been used as an adjuvant therapy after wide surgical excision or in those patients who have inoperable macroscopic disease. Postoperative radiotherapy has been associated with a cure rate of ?85 percent.[23] Ballo, et al., evaluated a combination of conservative resection and adjuvant radiation therapy and noted a local recurrence rate of 5 percent.[24] Risks of adjuvant radiotherapy include acute and chronic radiodermatitis and further development of new skin cancers.
Imatinib, a tyrosine kinase inhibitor, has been approved to treat adult patients with unresectable, recurrent, and/or metastatic disease. Imatinib inhibits the platelet-derived growth factor receptor tyrosine kinase and has been effective in treating DFSP in some patients despite CD117 negativity.[16,17]
The majority of local recurrences of DFSP occur within the first three years, with about half presenting within one year of surgery, but recurrences after five years have also been reported.[19,25] Thus, it is important to follow these patients over a long period after treatment.
In summary, we report a case of DFSP who presented clinically with a firm, violaceous, multinodular mass. The diagnosis was achieved on the basis of histological and immunohistochemical features. The patient decided to seek treatment from an oncologic surgeon and was lost to follow-up.
References
1. Gloster HM. Dermatofibrosarcoma protuberans. J Am Acad Dermatol. 1996;35:355–374.
2. Beech DJ, Long AB, Long WP. Dermatofibrosarcoma protuberans and breast cancer: genetic link or coincidental association? Am Surg. 2004;70(6):543–545.
3. Hoffman E. Uber das knollentreibende fibrosarkom de haut. Dermatol Z. 1925;43:1–28.
4. Stojadinovic A, Karpoff HM, Antonescu C, et al. Dermatofibrosarcoma protuberans of the head and neck. Ann Surg Oncol. 2000;7(9):696–704.
5. Criscione VD, Weinstock MA. Descriptive epidemiology of dermatofibrosarcoma protuberans in the United States, 1973 to 2002. J Am Acad Dermatol. 2007;56:968–973.
6. Asquo ME, Umoh MS, Ebughe G. Dermatofibrosarcoma protuberans: case reports. Ann Afr Med. 2007;6(2):80–83.
7. Reddy C, Hayward P, Thompson P, et al. Dermatofibrosarcoma protuberans in children. J Plast Reconstr Aesthet Surg. 2007;18[Epub].
8. Nouri K, Lodha R, Jimenez G, et al. Mohs micrographic surgery for dermatofibrosarcoma protuberans: University of Miami and NYU experience. Dermatol Surg. 2002;28(11):1060–1064.
9. Hanabusa M, Kamo R, Harada T, et al. Dermatofibrosarcoma protuberans with atrophic appearance at early stage of the tumor. J Dermatol. 2007;34(5):336–339.
10. Abrams TA, Schuetze SM. Targeted therapy for dermatofibrosarcoma protuberans. Curr Oncol Rep. 2006;8(4):291–296.
11. Mc Arthur G. Dermatofibrosarcoma protuberans: recent clinical progress. Ann Surg Oncol. 2007;14(10):2876–2886.
12. Behroozan DS, Glaich A, Goldberg LH. Dermatofibrosarcoma protuberans following tanning bed use. J Drugs Dermatol. 2005;4(6):751–754.
13. Abenoza P, Lillemoe T: CD34 and factor XIIIa in the differential diagnosis of dermatofibroma and dermatofibrosarcoma protuberans. Am J Dermatopathol. 1993;15:429–434.
14. Zelger BW, Ofner D, Zelger BG. Atrophic variants of dermatofibroma and dermatofibrosarcoma protuberans. Histopathology. 1995;26:519–527.
15. Mentzel T, Schärer L, Kazakov DV, et al. Myxoid dermatofibrosarcoma protuberans: clinicopathologic, immunohistochemical, and molecular analysis of eight cases. Am J Dermatopathol. 2007;29(5):443–448.
16. Fernandez-Flores A. Dermatofibrosarcoma protuberans is CD117 negative even after extreme antigen retrieval conditions. Rom J Morphol Embryol. 2007;48(4):419–421.
17. Labonte S, Hanna W, Bandarchi-Chamkhaleh B. A study of CD117 expression in dermatofibrosarcoma protuberans and cellular dermatofibroma. J Cutan Pathol. 2007;34(11):857–860.
18. Adler N, Tsabari C, Salkes J, et al. Cyclooxygenase-2 expression in dermatofibroma and dermatofibrosarcoma protuberans. J Cutan Pathol. 2008;14[Epub].
19. Ratner D, Thomas CO, Johnson TM, et al. Mohs micrographic surgery for the treatment of dermatofibrosarcoma protuberans. Results of a multi-institutional series with an analysis of the extent of microscopic spread. J Am Acad Dermatol. 1997;37:600–613.
20. Haycox CL, Odland PB, Olbricht SM et al. Dermatofibrosarcoma protuberans (DFSP): growth characteristics based on tumor modeling and a review of cases treated with Mohs micrographic surgery. Ann Plast Surg. 1997;38(3):246–251.
21. Thomas CJ, Wood GC, Marks VJ. Mohs micrographic surgery in the treatment of rare aggressive cutaneous tumors: the Geisinger experience. Dermatol Surg. 2007;33(3):333–339.
22. Snow SN, Gordon EM, Larson PO et. al. Dermatofibrosarcoma protuberans: a report on 29 patients treated by Mohs micrographic surgery with long-term follow-up and review of the literature. Cancer. 2004;101(1):28–38.
23. Mendenhall WM, Zlotecki RA, Scarborough MT. Dermatofibrosarcoma protuberans. Cancer. 2004;101(11):2503–2508.
24. Ballo MT, Zagars GK, Pisters P, et al. The role of radiation therapy in the management of dermatofibrosarcoma protuberans. Int J Radiat Oncol Biol Phys. 1998;40:823–827.
25. Ruiz-Tovar J, Fernàndez GM, Reguero CME et al. Dermatofibrosarcoma protuberans: review of 20-years experience. Clin Transl Oncol. 2006;8(8):606–610.