
Sharon E. Jacob, MD, Univeristy of Miami, Department of Dermatology and Cutaneous Surgery, Miami, Florida, University of California, San Diego, Division of Dermatology,
San Diego, California; Aparche Yang, MD, University of California–Los Angeles, Department of Pathology and Laboratory Medicine Division of Dermatopathology; Elise Herro, MD, University of California, San Diego, Division of Dermatology, San Diego, California; Chi Zhang, PhD, University of Miami, Director of Program Evaluation, Miami, Florida; Consultant (research methodology and statistical analyses)
Disclosure: The authors report no relevant conflicts of interest. Dr. Jacob has served as an investigator for Smarthealth USA on the PREA trial investigating the efficacy and safety of the TRUE test in children.
Abstract
Objective: The authors aimed to retrospectively identify associations between allergen sensitization frequencies and specific comorbidities in a patient population in Miami, Florida, tested between November 2004 and July 2006 with a pediatric standard series and to compare their findings to recent pediatric and adult patch testing data published by other North American referral centers. Design: The authors performed a retrospective chart review evaluating the most common, clinically relevant contact allergens against the frequency of specific comorbidities, such as atopic dermatitis. The results were compared with the patch testing data from the Ottawan Contact Dermatitis Group’s 1996–2006 study, the North American Contact Dermatitis Group 2001–2004 study, and the Mayo Clinic 1998–2000 study and the 2000–2006 study. Setting: University of Miami, Miami, Florida. Participants: Sixty-nine Miami children and adolescents between age six months and 18 years, having been referred for comprehensive patch testing. Measurements: The frequency of positive patch test reactions and clinical relevance was evaluated against the frequency of comorbidities. Results: Forty-five patients met all the inclusion criteria. Of these, 95.6 percent (43 patients) had at least one positive patch test reaction, with 76.7 percent of them having a personal history of atopic dermatitis. The most common pediatric allergens were found to significantly overlap with those of other North American referral centers. Conclusions: Allergic contact dermatitis is prevalent in atopic dermatitis; however, the authors were not able to demonstrate a statistically significant association, as the majority of patients referred had atopic dermatitis, and thus the control group was inadequate. Furthermore, allergens at the Miami center paralleled those seen at different centers within North America.
(J Clin Aesthet Dermatol. 2010;3(10):29–35.)
Allergic contact dermatitis (ACD) is a growing health complication in the pediatric population.[1–4] A significant prevalence of ACD in those with atopic dermatitis (AD) has been established in the literature.[5–8] The purpose of this study was to investigate associations between contact allergen sensitization and specific comorbidities (such as AD, asthma, or cigarette smoking in a household contact). In addition, the authors sought to compare their group data to the pediatric patch testing data published by another single referral center in North America, and to that of the consensus data from both adults and children tested in multicenter referral sites in North America.
METHODS
Patients. The authors performed a retrospective chart review of children evaluated for ACD at the University of Miami Pediatric Contact Dermatitis Clinic between November 2004 and July 2006. Of the 69 patients evaluated for ACD, 45 (65.2%) had met all the inclusion criteria: age six months to 18 years old; diagnosis of “rule out ACD” from the referring dermatologist, and comprehensive testing at the authors’ contact dermatitis referral center per previously described protocol.[9] Reasons documented in the charts for patch testing not being performed after initial evaluation included the following: the patient’s legal guardian had deferred patch testing; the procedure was not performable due to the extent of the patient’s dermatitis (too limited an area to patch test); and resolution of the patient’s dermatitis following initial consultation and patient adherence with the authors’ super-sensitive skin regimen (which includes instruction on skin barrier care and formaldehyde and fragrance avoidance).[9] Finally, one family refused to sign an informed consent, so patch testing was deferred by the center. The clinical diagnosis of AD was made according to the diagnostic criteria of Hanifin and Rajka.[10] Level of clinical relevance (definite, probable, possible, and past) was used as previously described.[11]
Data analysis. The frequencies of sensitization to clinically relevant contact allergens were evaluated against the frequencies of comorbidities, such as atopic dermatitis, asthma, hay fever, and household cigarette smoking. The authors’ patch testing results were compared to the pediatric patch testing data from the Ottawan 1996–2006 study period,[12] as well as both the adult and pediatric patch testing data from the North American Contact Dermatitis Group (NACDG) 2001–2004 study period and both the adult and pediatric patch testing data from the Mayo Clinic 1998–2000 and 2000–2006 study periods, respectively.[13–15]
Statistical analysis. Frequency tables were used to identify frequency of occurrence of each patient’s medical history as well as frequency of occurrence of all allergens. The two-sided Fischer’s exact test was used to determine the significance of the association between the comorbidity of a patient and his or her relevant allergen(s). A P value of less than 0.5 indicated a statistically significant difference. Statistical Package for the Social Sciences (SPSS) software was used for statistical analysis.
RESULTS
Data were reviewed for the 45 patients who were consecutively patch tested, aged 10 months to 16 years old (21 male and 24 female; mean age: 8.209±4.60 years; median age: 9 years). During this period, 69 children had been evaluated, 13 had deferred patch testing due to improvement on super-sensitive skin regimen (18.8%), seven were deferred (10.1%), and four were not tested due to the extensive nature of their dermatitis (5.8%). Of the 45 patients who had met the inclusion criteria, 95.6 percent (43 patients) had at least one positive patch test reaction. Two patients had negative patch tests. Of the 43 patients with positive patch tests, 76.7 percent (33 patients) had patch tests with definite or probable current clinical relevance and 22.2 percent (10 patients) had patch tests with possible current clinical relevance. Significant clinical improvement was noted after clinically relevant allergen avoidance in 93 percent of the patients in which definite or probable clinical relevance was determined.
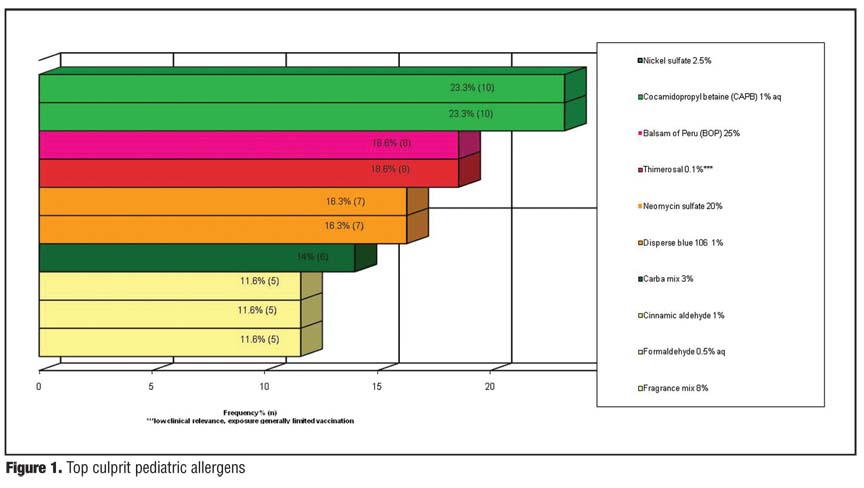
The most common, clinically relevant allergens were nickel (23.3%), cocamidopropyl betaine (CAPB, 23.3%), myroxylon pereirae (18.6%), neomycin (16.3%), disperse blue dye 106 (16.3%), carba mix (14%), cinnamic aldehyde (11.6%), formaldehyde (11.6%), and fragrance mix 1 (11.6%). These results are summarized in Figure 1 . Patient-specific comprehensive data for a subset of these patients tested between October 1, 2004, and May 1, 2006, are included in a report from a multicenter retrospective study.[11]
{kind=link}
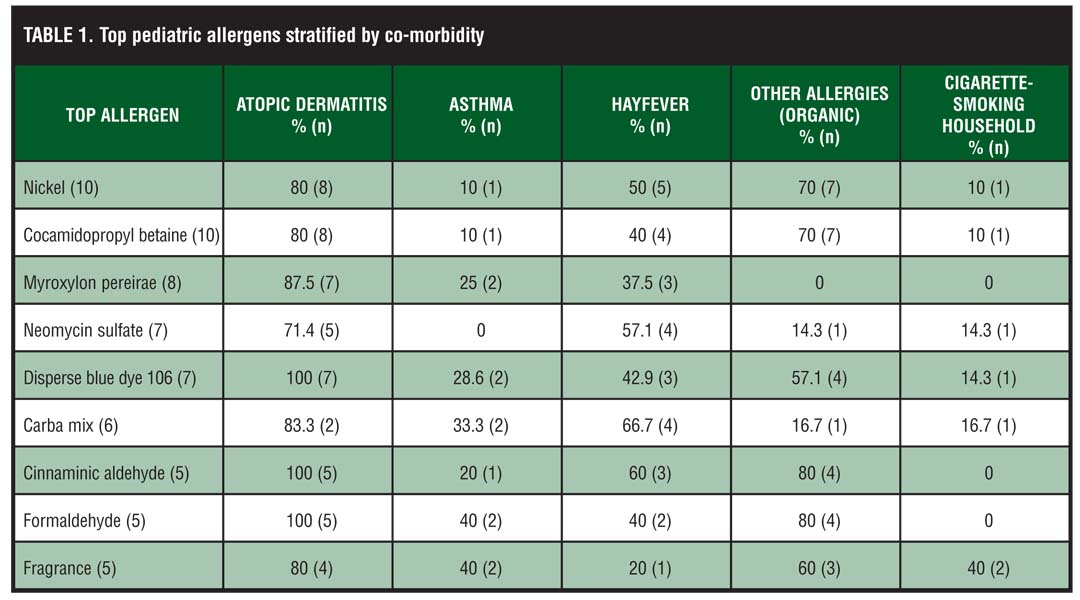
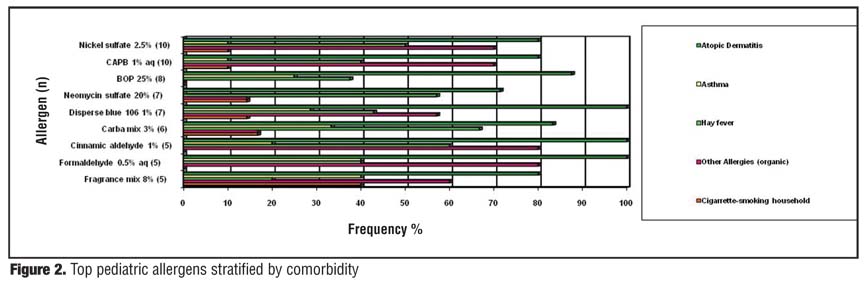
The authors’ evaluation of the frequency of contact allergen sensitization against the frequency of specific comorbidities showed no statistically significant associations, largely due to an inadequate control group at this referral institution. However, of the 43 patients with a positive patch test reading, 76.7 percent (33 patients) had a personal history of AD; 16.3 percent (7 patients) and 41.9 percent (18 patients) had a personal history of asthma and hay fever, respectively; and 48.8 percent (21 patients) had a history of a positive radioallergosorbent (RAST) or prick test to at least one allergen (e.g., eggs, grass, dust, cat dander, and dog dander). No children had a personal history of psoriasis, lupus, or thyroid disease. Five patients (11.6%) had at least one cigarette-smoking household contact, which did not correlate with allergen sensitization in this limited population. Both Table 1
and Figure 2
{kind=link}
{kind=link}
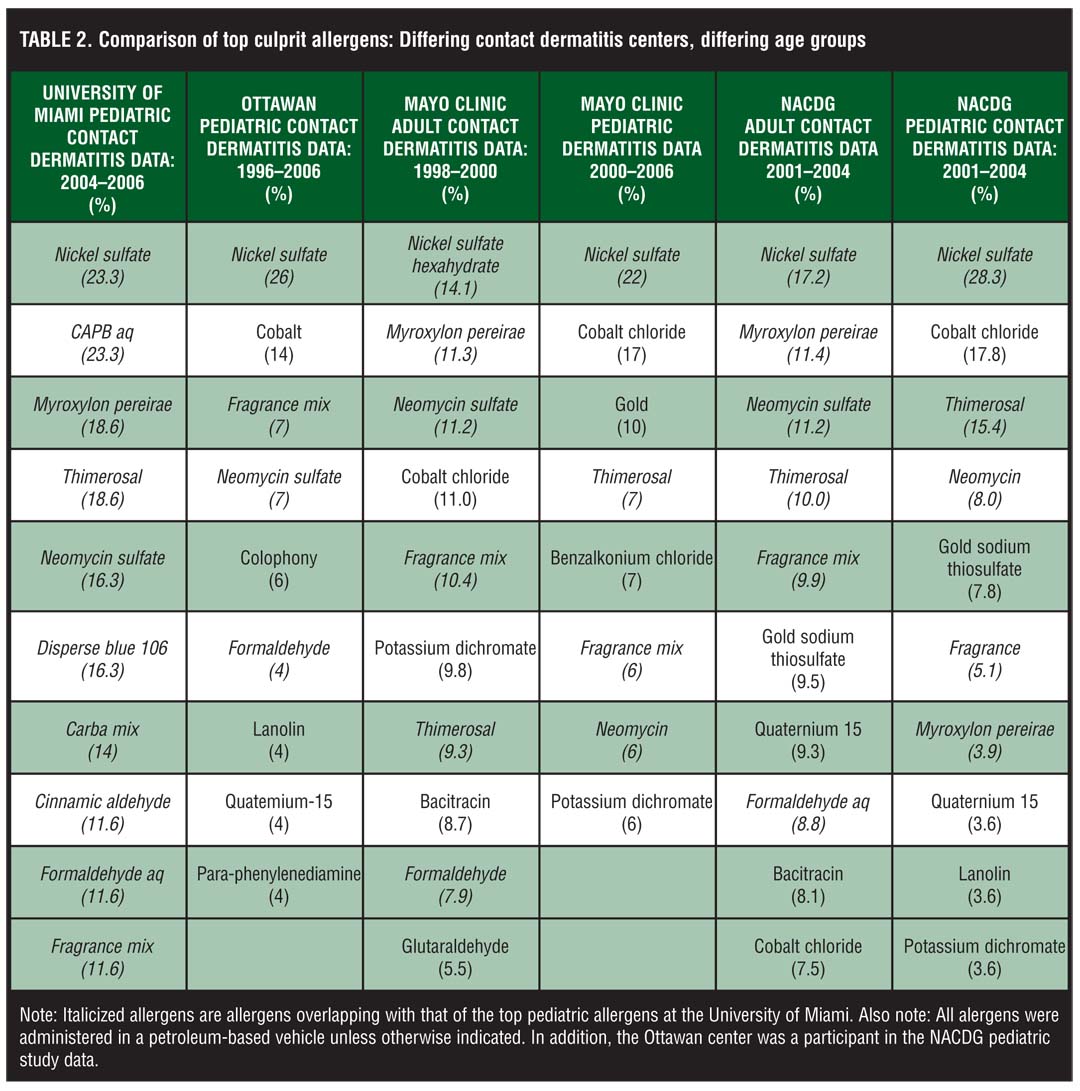
The top allergen frequencies reported in adult populations from both the Mayo Clinic and NACDG overlapped with six (nickel, myroxylon pereirae, neomycin, fragrance mix, thimerosal, formaldehyde) of the authors’ top pediatric allergens. Four (nickel, fragrance mix, neomycin, formaldehyde) of the Ottawan group’s top nine pediatric allergens overlapped with the authors’ top 10 pediatric allergens, nearly the same four allergens that overlapped from the Mayo Clinic’s pediatric top eight. Lastly, five (nickel, thimerosal, neomycin, fragrance mix, and myroxylon pereirae) of the NACDG’s top 10 pediatric allergens overlapped with the authors’ top 10 pediatric allergens. These results are summarized in Table 2.
{kind=link}
DISCUSSION
Variations in regional referral patterns, patch testing selection criteria, allergen exposure, and allergen testing may account for some of the differences in allergen frequencies reported by different referral centers.[1] The significant overlap of allergens in both pediatric and adult populations confirm that children and adults are being equally sensitized and developing ACD to similar environmental allergens.[2]
The authors notably were referred a significant number of patients who also carried the diagnosis of AD, resulting in 76.7 percent of the tested population of patients also carrying the diagnosis of AD (N=45, 2004–2006). While the authors recognize that this may overly suggest that an overwhelming number of patients with AD suffer from ACD, they do believe the actual clinical frequency of ACD in AD is high.[16]
A susceptibility to develop ACD in the setting of AD could be explained by the following: 1) the defective epidermal barrier may affect allergen absorption; 2) those with AD are chronically exposed to an array of sensitizers in skin care preparations intended to improve their condition; 3) a Th1 phenotype is added to the Th2 predominant milieu in the chronic eczematous phase of AD, which could contribute to contact allergen sensitization.[7,8,17] It is important to recognize that Th1 and Th2 hypersensitivity reactions are not mutually exclusive.[18] There is strong supporting evidence for a high proportion of patients with AD having a high incidence of immediate-type contact hypersensitivity, which can trigger their disease.[16,19,20] A recent German study linked AD and a loss-of-function filaggrin mutation to both immediate-type and delayed-type hypersensitivity reactions. This study examined patch test results of 1,537 people with both a history of AD and a loss-of-function filaggrin mutation.21 The study found a strong association between having AD, a loss-of-function filaggrin mutation, and nickel sensitization. Commentary for this article pointed out that nickel can induce both immediate and delayed hypersensitivity reactions.[22]
Nickel was found to be one of the top clinically relevant allergens in our population, matched by only CAPB in its prevalence. It was, however, the number one allergen reported in all of the compared studies in this manuscript, with its relevance as high as 26 percent.[15] And while classically nickel ACD presents on areas of greatest exposure, such as the earlobes, neck, and wrists (jewelry), and especially the infraumbilical area (jean snaps, belt buckles), it can also manifest as either an idiopathic or systemic reaction.[23] Idiopathic reactions are nonspecific dermatitic responses to allergens in sites that lack direct contact with the allergen, while a systemic response can manifest in a variety of ways. For example, patients can experience flares of previous patch test sites to vesicular hand dermatitis to symmetrical intertriginous and flexural exanthem, generalized dermatitis, exfoliative erythroderma, and oral lichenoid reactions following ingestion of their allergen.[24,25] Our experience with nickel sensitization (and improvement with dietary nickel avoidance) in patients with AD at the University of Miami Contact Dermatitis clinic has shown that the nickel reactions sometimes occur in a short time frame, suggesting the possibility that a more immediate reaction could be occurring in addition to a type IV delayed type hypersensitivity (and can be prevented). Given the ability of certain allergens to provoke both type I and IV reactions and the high incidence of both in patients with AD, the authors recommend including prick, RAST, and comprehensive patch test evaluation for patients with AD.[19]
As mentioned above, CAPB also ranked high in this patient population. CAPB is a surfactant commonly found in cleansers, foaming agents, and “no-tear” formulations. The rise in both the number of products containing this chemical (a 2,250% increase between 1980 and 2005) and the number of reported allergic reactions, led the American Contact Dermatitis Society (ACDS) to name it the Allergen of the Year in 2004.[26] The high prevalence of this allergen in patients with AD (76.7%), and the potential for a significant number of irritant reactions to this allergen, led the authors to question the validity of their results. For this reason, the authors evaluated the correlation of CAPB positivity with amidoamine and/or dimethylamino-propylamine (DMAPA), concomitant provocative testing data, and the improvement of the patients with avoidance. Their findings supported that these were indeed true positive reactions.
Next, the prevalence of ACD to myroxylon pereirae and thimerosal were equal and paralleled the high rank reported in the Mayo Clinic and NACDG adult contact dermatitis studies. In addition, fragrance mix 1 (which contains 3 myroxylon pereirae-based chemicals, specifically cinnamic aldehyde) ranked in the top 10 of all the studies reviewed in this paper. Notably, myroxylon pereirae is a dark brown, complex, viscous fluid harvested from the wounded mature myroxylon pereirae tree. It has wide utilization by pharmaceutical, perfume, cosmetic, and flavoring industries. An increasing number of ACD reactions to myroxylon pereirae and fragrances have been seen in infancy and childhood, likely due to the large variety of baby care products that contain derivatives of the extract or cross-reactors, many of which are applied under occlusion to the diaper area.[27]
Thimerosal is a mercuric derivative of thiosalicyclic acid that has been used as a disinfectant and a preservative in some vaccines, cosmetics, tattoo inks, eye drops, and contact lens solutions. While thimerosal continually is cited as possessing a high sensitizing capacity, its low clinical relevance (e.g., positive patch tests not associated with the current presenting dermatitis) has led to it no longer being included on most tertiary care centers’ standard panels. The only vaccine recommended for children under seven years of age that still contains thimerosal is the inactivated influenza vaccine.[28,29]
Neomycin, a well-known antibiotic ointment and cream, ranked among the top 10 in all the studies evaluated in this review. Of interest, neomycin has been one of the most prevalent sensitizers in adult populations for the last three decades, second only to nickel. The sensitization rates in children have increased as well, likely from both the over-the-counter availability and utilization patterns of these products for minor injuries and “superinfections,” especially in the atopic population.[28] In 2010, neomycin was designated Contact Allergen of the Year by the ACDS.[28,30] While many patients with antibiotic allergy present with dermatitis at the site of product application,[31] the topical application of both neomycin and bacitracin have been reported to induce anaphylactic reactions as well.[31–33]
Disperse blue dye 106 was another top clinically relevant allergen noted in this study. Disperse dyes are primarily used to color polyester, acetate, and nylon fibers and are the most common dye sensitizers due to their partial water solubility, resulting in significant leaching out of fabrics with normal wear and with repeated garment washing, ultimately causing absorption by the skin. In two studies published in 2000, 18 and 40 percent of the patients suspected of having a textile ACD had positive patch tests to textile dyes (with the most common allergens being disperse blue 124, disperse blue 106, and disperse blue 85).[34,35] The rise in prevalence of this allergen led to disperse dyes being designated as the 2000 Contact Allergen of the Year. In a 2003 study of 1,098 children, Giusti et al reported a sensitization rate of 4.6 percent to disperse dyes, with 59 percent of these children having AD or a history of AD.[36] Children with AD may have been more likely to have this allergy due to their impaired skin barrier, providing an easier portal of entry when in contact with clothing. Notably, in this study, the most common sensitizer was disperse yellow 3, followed by disperse orange 3, and disperse blue 124.[36]
Lastly, formaldehyde placed on the top 10 list in this study’s data and three of the studies the authors compared in this manuscript—the Ottawan pediatric, Mayo Clinic adult, and the NACDG adult CD studies. Formaldehyde is found in clothing, building materials, and many personal hygiene products, used as both a preservative and for its antimicrobial properties.[30,37] The authors acknowledge that, in fact, they may have inadvertently underestimated the prevalence rate of formaldehyde (and fragrances) with the implementation of their “super sensitive skin regimen,” which includes the avoidance of these agents in patients with moderate-to-severe dermatitis.[9] Notably, 18 percent of the 69 evaluated children experienced significant improvement of their dermatitis with the implementation of the regimen alone and led to deference of the patch test. Ultimately, this may have led the authors to under report the frequency of these allergens in the patient population.
There are several limitations to this study, including the inherent limitations of a retrospective review, the low statistical power of a small patient population, and the referral bias of a tertiary care center with a patient population characterized by refractory, moderate-to-severe dermatitis. The authors recognize that this study represented a subset of children specifically referred by dermatologists for evaluation of ACD and may not be applicable to the pediatric population at large. This study demonstrates a need for additional multicenter, prospective studies incorporating sites from multiple regions.
Acknowledgment
The authors would like to acknowledge Carmen Gelpi; Israel Borrego; Antoine Amado, MD; Tace Steele, MD; and Mari Paz Castanedo-Tardan, MD, for their dedication to patient care and assistance in the evaluation of the patients presented in this study.
References
1. Beattie PE, Green C, Lowe G, Lewis-Jones MS. Which children should we patch test? Clin Exp Dermatol. 2007;32(1):6–11. Epub 2006 Sep 27.
2. Militello G, Jacob SE, Crawford GH. Allergic contact dermatitis in children. Curr Opin Pediatr. 2006;18(4): 385–390.
3. Bruckner AL, Weston WL. Allergic contact dermatitis in children: a practical approach to management. Skin Therapy Lett. 2002;7(8):3–5.
4. Onder M, Adisen E. Patch test results in a Turkish paediatric population. Contact Dermatitis. 2008;58(1):63–65.
5. Cronin E, Bandmann HJ, Calnan CD, et al. Contact dermatitis in the atopic. Acta Derm Venereol. 1970;50:183–187.
6. Marghescu S. Patch test reactions in atopic patients. Acta Derm Venereol. 1985;114 (suppl):113–116.
7. Lammintausta K, Kalimo K, Fagerlund VL. Patch test reactions in atopic patients. Contact Dermatitis. 1992;26: 234–240.
8. Lugovic L, Lipozencic J. Contact hypersensitivity in atopic dermatitis. Arh Hig Rada Toksikol. 1997;48:287–296.
9. Jacob SE, Burk CJ, Connelly EA. Patch testing: another steroid-sparing agent to consider in children. Pediatr Dermatol. 2008;25(1):81–87.
10. Hanifin KM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol. 1980;92:44–47.
11. Jacob SE, Brod BA, Crawford GH. Clinically Relevant Patch Test Reactions in Children—A United States Based Study. Pediatr Dermatol. 2008;25(5):520–527.
12. Hogeling M, Pratt M. Allergic contact dermatitis in children: the Ottawa hospital patch-testing clinic experience, 1996 to 2006. Dermatitis. 2008;19(2):86–89.
13. Wetter DA, Davis MDP, Yiannias JA, et al. Patch test results from the Mayo Clinic Contact Dermatitis Group, 1998–2000. J Am Acad Dermatol. 2005;53(3):416–421.
14. Pratt MD, Belsito DV, DeLeo VA, et al. North American Contact Dermatitis Group patch-test results, 2001–2002 study period. Dermatitis. 2004;15(4):176–183.
15. Zug KA, McGinley-Smith D, Warshaw EM, et al. Contact Allergy in Children Referred for Patch Testing: North American Contact Dermatitis Group Data, 2001–2004. Arch Dermatol. 2008;144(10):1329–1336.
16. Oranje AP, Bruynzeel DP, Stenveld HJ, Dieges PH. Immediate and delayed contact hypersensitivity in children older than 5 years with atopic dermatitis: a pilot study comparing different tests. Pediatr Dermatol. 1994;11:209–115.
17. Belhadjali H, Mohamed M, Youssef M, et al. Contact sensitization in atopic dermatitis: results of a prospective study of 89 cases in Tunisia. Contact Dermatitis. 2008;58(3):188–189.
18. Wüthrich B, Cozzio A, Roll A, et al. Atopic eczema: genetics or environment? Ann Agric Environ Med. 2007;14(2):195–201.
19. Usmani N, Wilkinson SM. Allergic skin disease: investigation of both immediate- and delayed-type hypersensitivity is essential. Clin Exp Allergy. 2007;37(10):1541–1546.
20. Purohit-Sheth TS, Carr WW. Oral allergy syndrome (pollen-food allergy syndrome). Allergy Asthma Proc. 2005;26: 229–230.
21. Novak N, Baurecht H, Schäfer T, et al. Loss-of-function mutations in the filaggrin gene and allergic contact sensitization to nickel. J Invest Dermatol. 2008;128(6): 1430–1435. Epub 2007 Nov 29.
22. Hanifin JM. Filaggrin mutations and allergic contact sensitization. J Invest Dermatol. 2008;128(6):1362–1364.
23. Hsu JW, Matiz CM, Jacob SE. Nickel Allergy: localized, Id, and systemic manifestations in children. Pediatr Dermatol. 2010; in press.
24. Nijhawan RI, Molenda M, Zirwas MJ, Jacob SE. Systemic contact dermatitis. Dermatol Clin. 2009;27:355–364.
25. Szyfelbein Masterpol K, Gottlieb AB, Scheinman PL. Systemic contact dermatitis presenting as lichen planus of the lip. Dermatitis. 2010;21:218–219.
26. Jacob SE, Amini S. Cocamidopropyl betaine. Dermatitis. 2008;19(3):157–60. Review.
27. Hausen BM. Contact allergy to balsam of Peru. II. Patch test results in 102 patients with selected balsam of Peru constituents. Am J Contact Dermat. 2001;12(2):93–102.
28. Nijhawen RI, Matiz C, Jacob SE. Contact dermatitis: from basics to allergodromes. Pediatric Annals. 2009;38(2): 99–108.
29. Breithaup A, Jacob SE. Thimerosal and the relevance of patch-test reactions in children. Dermatitis. 2008;19(5): 275–277.
30. Jacob SE, Breithaupt A. Environmental exposures—a pediatric perspective on allergic contact dermatitis. Skin & Aging. 2009 July;28–36.
31. Holden CR, Gawkrodger DJ. 10 years’ experience of patch testing with a shoe series in 230 patients: which allergens are important? Contact Dermatitis. 2005;53(1):37–39.
32. Cronin H, Mowad C. Anaphylactic reaction to bacitracin ointment. Cutis. 2009;83(3):127.
33. Agathos M. Anaphylactic reaction to framycetin (neomycin B) and lignocaine. Contact Dermatitis. 1980;6(3):236–237.
34. Pratt M, Taraska V. Disperse blue dyes 106 and 124 are common causes of textile dermatitis and should serve as screening allergens for this condition. Am J Contact Dermat. 2000;11:30–41.
35. Lazarov A, Trattner A, David M, Ingber A. Textile dermatitis in Israel: a retrospective study. Am J Contact Dermat. 2000;11:26–29.
36. Giusti F, Massone F, Bertoni L, et al. Contact sensitization to disperse dyes in children. Pediatr Dermatol. 2003;20(5): 393–397.
37. Moennich JN, Hanna DM, Jacob SE. Formaldehyde-releasing preservative in baby and cosmetic products: health risks related to exposure during infancy. Journal of Dermatology Nursing. 2009;1(3):211–214.