
Amylynne J. Frankel, MD, Mount Sinai Medical Center, New York, New York; Joshua A. Zeichner, MD, Assistant Professor of Dermatology, Mount Sinai Medical Center, New York, New York; James Q. Del Rosso, DO, FAOCD, Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada
Disclosure: Dr. Frankel reports no relevant conflicts of interest. Dr. Zeichner is a consultant for Promius. Dr. Del Rosso is a consultant, speaker, and or researcher for Allergan, Coria, Galderma, Graceway, Intendis, Leo Pharma, Medicis, Onset Therapeutics, Ortho Dermatology, PharmaDerm, Promius, Quinnova, Ranbaxy, SkinMedica, Stiefel, Triax, Unilever, and Warner Chilcott.
Abstract
Psoriasis is a chronic, inflammatory, immune-mediated, multi-system disease that is treated with a variety of medicines, including topical corticosteroids and, historically, coal tar. In this case, the authors evaluated whether combination therapy with coal tar foam 2% and a topical corticosteroid would induce a remission and maintain clearance of plaque-type psoriasis over an eight-week period. A 59-year-old Caucasian woman with plaque psoriasis of her elbows presented to the authors’ dermatology clinic and was treated with clobetasol propionate 0.05% emollient foam in combination with coal tar 2% foam twice daily to her elbows for two weeks. After two weeks, the patient was switched to a maintenance regimen of twice-daily coal tar 2% foam during the week and twice-daily application of the corticosteroid on the weekends. The patient exhibited very favorable clearance of her plaque psoriasis on this regimen at her eight-week follow-up visit. In this case, the combination of coal tar 2% foam and clobetasol propionate 0.05% emollient foam twice daily was used effectively to induce remission of localized plaque psoriasis followed by an efficacious maintenance regimen, which incorporated intermittent therapy with both topical agents. (J Clin Aesthet Dermatol. 2010;3(10):42–45.)
Psoriasis is a chronic, inflammatory, immune-mediated, multi-system disease with a prevalence of approximately 1 to 3 percent worldwide.[1] Chronic plaque psoriasis, or psoriasis vulgaris, is the most common form of the disease, accounting for 85 to 90 percent of cases. Joint involvement is common, affecting anywhere from 6 to 42 percent of patients with psoriasis.[2] Other phenotypes include intertriginous, scalp, palmar, plantar, and seborrheic variants, and patients may present with multiple clinical forms.[3] At present, there is no curative therapy available and the clinical course is typically chronically remitting and relapsing disease with well circumscribed, erythematous, indurated plaques with scale.[4] The goal of psoriasis therapy is to gain initial and rapid control of the disease, decrease body surface area involved, and achieve long-term remission using an approach that is effective, safe, and convenient.[5,6] Topical therapies often constitute first-line treatment for mild-to-moderate skin disease that is localized and are associated with minimal adverse events provided patients are appropriately monitored.[7] Treatment selection is determined by the severity and location of the psoriasis as well as medication side effects, patient preferences, and financial constraints. Topical therapies are the most common agents for the treatment of psoriasis in the United States and are used as monotherapy or in combination with other medications depending on the needs of the individual case.[8]
Careful selection of both class of medication and its vehicle is crucial in the treatment of psoriasis. Commonly used topical medications for psoriasis include corticosteroids, vitamin D analogues, keratolytics, anthralin, coal tar, and tazarotene.[4] Topical medications are used by approximately 85 percent of patients with psoriasis and most often provide favorable response rates with good overall safety profiles.[8] Topical corticosteroids are usually considered a first-line therapy for localized plaque psoriasis. They are available in varying strengths and formulations and may be used individually or in various combinations.[4,9–11] Monotherapy with one of the medicines mentioned above may not be efficacious, especially with more prolonged use, or may produce unwanted side effects, especially when applied chronically.[6] Combination, rotational, and sequential regimens with topical corticosteroids and other medications can help control psoriasis while also reducing the risk of potential side effects.[6]
There are many benefits to combination therapy for psoriasis. A meta-analysis of 22 studies reported that clearing rates following monotherapy ranged from 2 to 85 percent versus clearance rates of 39 to 100 percent for combination therapies.[5] Combination therapies use two or more therapeutic agents at once to optimize their effectiveness. Lower doses of individual agents may be used with the potential for additive therapeutic effects of the two (or more) medicines. Rotational regimens use a single agent for a specific amount of time before switching to another agent. The goal is to prevent toxic doses or side effects and lack of effectiveness over time, which is common with topical monotherapy. Sequential treatments involve the use of a potent medication for a short period of time, which is then replaced or combined with other drugs to lower the dose of the more toxic drug.[12]
Coal tar is a resin that has been used topically for dermatological conditions for more than 2,000 years.[13] The use of coal tar has declined in Western countries for various reasons, including unappealing color, odor, ability to stain clothing, and questionable carcinogenicity. However, it is still considered a first-line therapy in many parts of the world.[6] Today, some new vehicles have been developed that provide improved penetration and/or cosmetic acceptability of coal tar. The following case demonstrates the use of topical coal tar 2% foam in combination with a superpotent topical corticosteroid foam for the treatment of psoriasis. Coal tar 2% foam in combination with clobetasol propionate 0.05% emollient foam used for treatment of plaque psoriasis of the elbows was effective in inducing a remission with concurrent use and subsequently maintaining clearance with an intermittent therapy approach.
Case Presentation
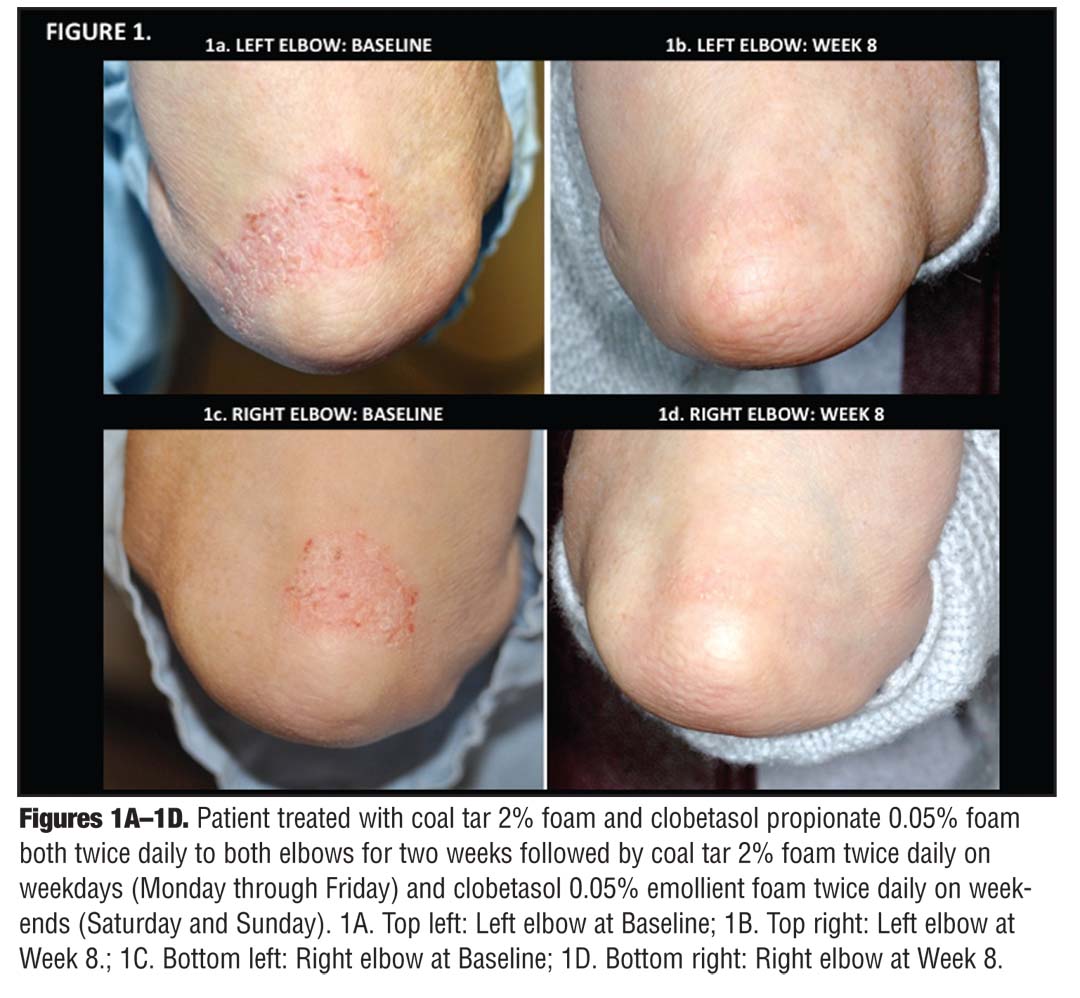
A 59-year-old Caucasian woman presented to the clinic for the treatment of long-standing plaque-type psoriasis. On physical examination, she had moderate plaque-type psoriasis affecting her bilateral elbows, palms, and soles. The patient had no signs or symptoms of arthritis and was otherwise healthy, taking no medications. She had no known drug allergies and was postmenopausal. The patient was given two products, clobetasol propionate 0.05% emollient foam and coal tar 2% foam and instructed to use both twice daily on her elbows for two weeks. After two weeks, the patient was switched to a maintenance regimen of twice-daily coal tar 2% foam applied during the week (Monday through Friday) and twice-daily corticosteroid foam applied on the weekends (Saturday and Sunday). On follow-up visit at Week 8, the plaques were significantly improved ( Figures 1A–1D ). The patient had no complaints with either the coal tar foam or the corticosteroid foam and did not report any side effects. The clinicians who examined the patient observed no adverse effects.
{kind=link}
Discussion
Topical corticosteroids are the most commonly used topical agents for the treatment of psoriasis, but are associated with the potential for clinically relevant side effects with long-term use. Combination therapy with nonsteroidal medications has been developed to minimize the side effects associated with long-term topical corticosteroid therapy. Moreover, clinical trials evaluating various topical therapies in combination with topical corticosteroids have demonstrated improved clinical benefit compared with topical corticosteroid monotherapy.[12,14–15] Despite being a more simple regimen, topical corticosteroid monotherapy may not be efficacious when used on a prolonged basis for a variety of reasons, including cutaneous adverse effects and loss of efficacy.[15]
Tars are resins comprising a myriad of different compounds.[16] Coal tar has been employed for psoriasis both as monotherapy and in combination with other topical agents, systemic medicines, and phototherapy.[17] Indeed, in 1681 Becher and Serle documented the use of crude coal tar for dermatological diseases, and in 1895 Kaposi noted that tar was an important part of his pharmacopoeia.[18] The utilization of coal tar was popularized by its effective use in combination with ultraviolet B (UVB) phototherapy, first as part of the original Goeckerman regimen and later in modified regimens.[18-22] The Goeckerman regimen is performed on an inpatient basis, is safe and reliable, and results in long-germ remissions, even in patients unresponsive to other conventional therapies.
The mechanism of action of coal tar is not well understood. Postulated effects include a suppression of deoxyribonucleic acid (DNA) synthesis and subsequent inhibition of keratinocyte proliferation.[18,23] Coal tar is thought to help correct the defect of differentiation in keratinocytes of psoriatics. Additionally, it may possess antimicrobial as well as anti-inflammatory and antipruritic effects.[18] Thus, the modes of action of tar may function in an additive manner with topical corticosteroids, which have anti-inflammatory, immunosuppressive, and antipruritic properties.
Coal tar exists in various preparations including crude coal tar, coal tar ointment, coal tar solution, and coal tar shampoos. Currently, the use of coal tar is reserved mainly for patients with chronic plaque psoriasis, scalp psoriasis, atopic dermatitis, seborrheic dermatitis, and neurodermatitis.[18] Historically, coal products have been poorly tolerated by patients for several reasons. Cosmetic concerns include staining of the clothing as well as a malodorous tar smell. Medical side effects also occur, such as irritant contact dermatitis, folliculitis, and UVA photosensitivity.[9] Additionally, there have been concerns that coal tar has led to an increase in carcinogenicity; however, there is inconclusive evidence that this is the case.[18,24] While coal tar is not used commonly in the United States, in other parts of the world it is considered to be first-line topical therapy, especially for plaque psoriasis.[13]
Coal tar 2% foam (Scytera® Foam, Promius Pharma, LLC, Bridgewater, New Jersey) is a novel coal tar formulation in an aerosol foam vehicle. It is a “behind-the-counter” product at the pharmacy, which may be obtained by the patient with a recommendation from the physician, but without a prescription. This formulation has been designed differently from previous vehicle forms of coal tar in that the emollient foam spreads easily and dries quickly into skin, with minimal odor from coal tar. Due to its rapid penetration and disappearance into skin, effectiveness may be more achievable as adherence is more likely with a topical agent that is more easily applied, is not messy, and is cosmetically acceptable to the patient. With regard to the efficacy of coal tar in psoriasis, crude coal tar ointment, with or without a topical corticosteroid under occlusion, has been reported to be efficacious.[18,25]
In conclusion, in the described case report, coal tar 2% foam was used effectively in combination with a clobetasol propionate 0.05% emollient foam. Previous tar-containing products have not been widely accepted due to their unpleasant odor, messy nature, and/or staining of hair, skin, and clothing.[6] However, in this case, coal tar 2% foam did not result in any adverse events or deter the patient with regard to cosmetic acceptability of the product. Coal tar 2% foam may be a promising addition to the armamentarium of medications available for psoriasis patients and appears to be applicable for use in combination with a topical corticosteroid.
References
1. van de Kerkhof PC, Franssen ME. Psoriasis of the scalp. Diagnosis and management. Am J Clin Dermatol. 2001;2(3): 159–165.
2. Gottlieb A, Korman NJ, Gordon KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 2. Psoriatic arthritis: overview and guidelines of care for treatment with an emphasis on the biologics. J Am Acad Dermatol. 2008;58(5): 851–864.
3. Farley E, Masrour S, McKey J, Menter A. Palmoplantar psoriasis: a phenotypical and clinical review with introduction of a new quality-of-life assessment tool. J Am Acad Dermatol. 2009;60(6): 1024–1031.
4. Sukarovska BG, Lipozencic J, Vrzogic P. [Topical corticosteroids and corticosteroid sparing therapy in psoriasis management]. Acta Med Croatica. 2007;61(4):375–381.
5. Lebwohl M, Kathryn M. New roles for systemic retinoids. J Drugs Dermatol. 2006.5(5):406–409.
6. Lebwohl M. A clinician’s paradigm in the treatment of psoriasis. J Am Acad Dermatol. 2005;53(1 Suppl 1): S59–S69.
7. Kamili QU, Menter A. Topical treatment of psoriasis. Curr Probl Dermatol. 2009;38:37–58.
8. Gold LF. Calcitriol ointment: optimizing psoriasis therapy. J Drugs Dermatol. 2009;8(8 Suppl):S23–S27.
9. Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. Section 3. Guidelines of care for the management and treatment of psoriasis with topical therapies. J Am Acad Dermatol. 2009;60(4):643–659.
10. Koo JY. Using topical multimodal strategies for patients with psoriasis. Cutis. 2007;79(1 Suppl 2):11–17.
11. Stein Gold L, Corvari L. The roles of safety and compliance in determining effectiveness of topical therapy for psoriasis. Cutis. 2007;79(1 Suppl 2):32–38.
12. Koo JY. New developments in topical sequential therapy for psoriasis. Skin Therapy Lett. 2005;10(9):1–4.
13. Roelofzen JH, Aben KK, Khawar AJ, et al. Treatment policy for psoriasis and eczema: a survey among dermatologists in the Netherlands and Belgian Flanders. Eur J Dermatol. 2007;17(5):416–421.
14. van der Velden HM, Pasch MC, van Erp PE, et al. Treatment of plaque psoriasis with the two-compound product calcipotriol/betamethasone dipropionate versus both monotherapies: an immuno-histochemical study. J Dermatolog Treat. 2010;21(1):13–22.
15. Lebwohl M, Menter A, Koo J, Feldman SR. Combination therapy to treat moderate to severe psoriasis. J Am Acad Dermatol. 2004;50(3):416–430.
16. Arnold WP. Tar. Clin Dermatol. 1997;15(5):739–744.
17. Pardasani AG, Feldman SR, Clark AR. Treatment of psoriasis: an algorithm-based approach for primary care physicians. Am Fam Physician. 2000;61(3):725–733, 736.
18. Paghdal KV, Schwartz RA. Topical tar: back to the future. J Am Acad Dermatol. 2009;61(2):294–302.
19. Silverman A, Menter A, Hairston JL. Tars and anthralins. Dermatol Clin. 1995;13(4):817–833.
20. de Rie MA, Out TA, Bos JD. Low-dose narrow-band UVB phototherapy combined with topical therapy is effective in psoriasis and does not inhibit systemic T-cell activation. Dermatology. 1998;196(4):412–417.
21. Davis MD, McEvoy MT, Camilleri M, et al. Goeckerman treatment: neglected in the consensus approach for critically challenging case scenarios in moderate to severe psoriasis. J Am Acad Dermatol. 2010;62(3):508.
22. de Miguel R, el-Azhary R. Efficacy, safety, and cost of Goeckerman therapy compared with biologics in the treatment of moderate to severe psoriasis. Int J Dermatol. 2009;48(6):653–658.
23. Smith CH, Jackson K, Chinn S, Angus K, Barker JN. A double blind, randomized, controlled clinical trial to assess the efficacy of a new coal tar preparation (Exorex) in the treatment of chronic, plaque type psoriasis. Clin Exp Dermatol. 2000;25(8):580–583.
24. Roelofzen JH, Aben KK, Oldenhof UT, et al. No increased risk of cancer after coal tar treatment in patients with psoriasis or eczema. J Invest Dermatol. 2010;130(4):953–961.
25. Kumar B, Kumar R, Kaur I. Coal tar therapy in palmoplantar psoriasis: old wine in an old bottle? Int J Dermatol. 1997;36(4):309–312.