
Stephanie J. Martin, BA, Medical School, The University of Texas Medical School at Houston, Houston, Texas; Philip R. Cohen, MD, Department of Dermatology, University of Texas MD Anderson Cancer Center, Houston, Texas, Department of Dermatology, University of Texas Medical School at Houston, Houston, Texas, University of Houston Health Center, University of Houston, Houston, Texas; Jeong Hee Cho-Vega, MD, PhD, St. Joseph Dermpath, Houston, Texas; Jaime A. Tschen, MD, Medical School, The University of Texas Medical School at Houston, Houston, Texas, St. Joseph Dermpath, Houston, Texas.
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Background: Pagetoid reticulosis is a rare variant of mycosis fungoides. This rare condition typically presents as a solitary plaque located on the extremities with an indolent clinical course (Woringer-Kolopp disease) or as a more generalized presentation with diffuse cutaneous involvement and a more aggressive clinical course (Ketron-Goodman disease). Purpose: To review the cutaneous manifestations, pathology, and treatment of localized pagetoid reticulosis. Methods: The authors describe a 24-year-old woman with a slowly enlarging, localized plaque of seven months duration, representing the localized form of pagetoid reticulosis with CD8+ immunophenotype. Results: The histological, immunohistochemical, and clinical features of the patient’s skin lesion were characteristic for a diagnosis of Woringer-Kolopp disease. Systemic work-up for lymphoma was negative. Conclusion: Woringer-Kolopp disease is most commonly seen in middle-aged men as a solitary lesion of the extremities, and it should always be considered in the differential diagnosis when a patient presents with such a lesion. A histological analysis demonstrated atypical lymphocytes preferentially localized to the epidermis with a CD4+, CD8+, or CD4-/CD8- phenotype. The treatment of choice for a solitary lesion may be localized radiation therapy, but newer therapies, such as bexarotene, may warrant further investigation. (J Clin Aesthet Dermatol. 2010;3(10):46–49.)
Pagetoid reticulosis is defined by the World Health Organization-European Organization for the Research and Treatment of Cancer (WHO-EORTC) as a variant of mycosis fungoides.[1,2] This skin disorder is characterized by an intraepidermal proliferation of atypical lymphocytes that can present either as a solitary hyperkeratotic patch confined to a localized area or as a more generalized lesion with diffuse cutaneous involvement.[3] Localized pagetoid reticulosis is known as Woringer-Kolopp disease, and generalized pagetoid reticulosis is known as Ketron-Goodman disease.[4] The authors describe a 24-year-old woman with a slowly enlarging, localized plaque of seven months duration, demonstrating the Woringer-Kolopp disease variant of pagetoid reticulosis, containing a predominance of CD8+ T-cells.
Case Report
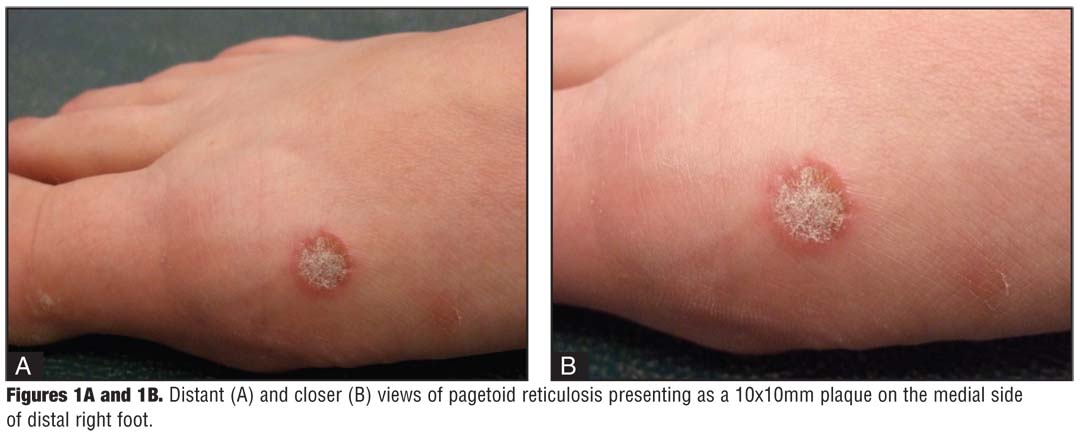
A 24-year-old woman from Finland presented for evaluation of a 10x10mm, erythematous plaque with central scaling and a raised border on the medial side of the distal right foot (Figure 1). The lesion initially appeared seven months earlier and had been slowly enlarging. Examination of the skin and the oral mucosa showed no other lesions. A 3mm punch biopsy was performed and submitted for routine histopathological evaluation.
{kind=link}
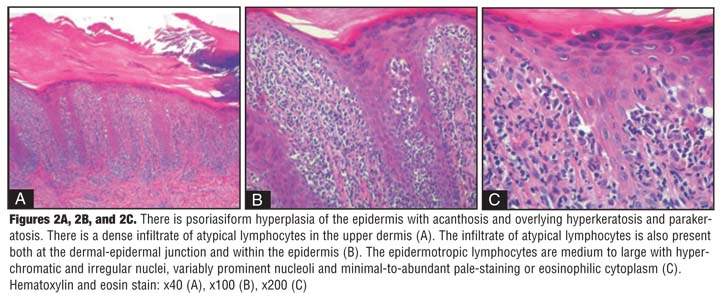
Histological sections showed an epidermis with hyperkeratosis and parakeratosis in association with acanthosis, which adopted a psoriasiform appearance at low magnification (Figure 2A). A dense infiltrate of atypical lymphocytes in the papillary dermis (Figure 2B) and an extensive intraepidermal infiltrate of atypical lymphocytes were reported. The groups of tumor cells in the epidermis demonstrated Pautrier microabcess-like configuration. The epidermotrophic atypical lymphocytes were medium to large with hyperchromatic and irregular nuclei, variably prominent nucleoli, and minimal-to-abundant pale-staining or eosinophilic cytoplasm (Figure 2C). Some of the cells showed a perinuclear halo. Rare mitotic figures were also observed. Focally, the basement membrane region of the epidermis was intact and clearly demarcated (Figure 2C). The reticular dermis contains a sparse perivascular lymphohistiocytic infiltrate in which the atypical lymphocytes are rarely seen.
{kind=link}
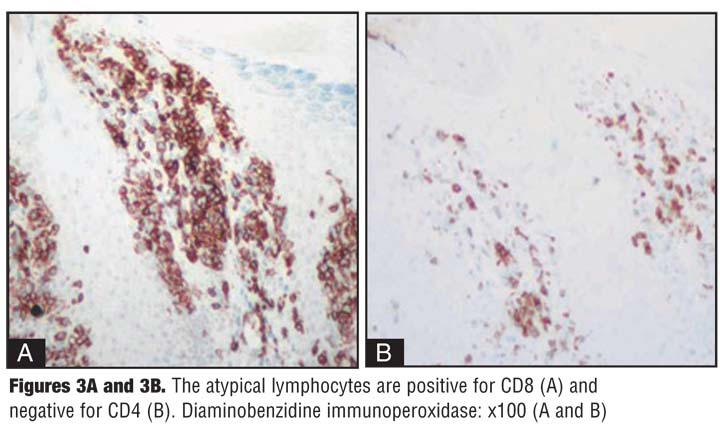
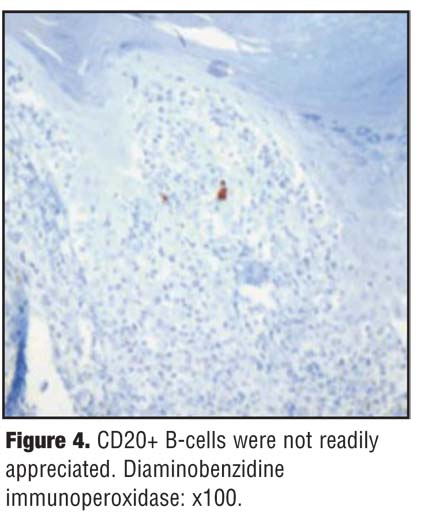
Immunohistochemical studies performed on paraffin sections revealed that the neoplastic cells were positive for CD3 (T-cells) and CD8 (suppressor/cytotoxic T-cells) (Figure 3A) and negative for CD4 (helper T-cells) (Figure 3B). A dense infiltrate, with reactive CD4+ T-cells, was observed in the upper dermis (Figure 3B). Almost all of the neoplastic cells had lost CD7 expression. CD20+ B-cells were not readily identified (Figure 4).
{kind=link}
{kind=link}
The histological, immunohistochemical, and clinical features of the patient’s lesion were most consistent with a diagnosis of solitary pagetoid reticulosis. Systemic work-up for lymphoma was negative.
The patient decided to return to Finland for treatment. The same pathology was observed after an excisional biopsy, removing the entire residual lesion, was performed to confirm the diagnosis. Radiation therapy was recommended if the tumor recurs.
Discussion
Woringer and Kolopp first described the clinical features of pagetoid reticulosis in 1939[5] in a case of a 13-year-old boy presenting with a solitary, erythematous, scaly patch on his forearm.[6] On histological examination, there were cells with basophilic nuclei and scant cytoplasm grouped in nests in the epidermis.[7] The name Woringer-Kolopp disease was later coined by Braun-Falco et al in 1973.[8]
Ketron and Goodman originally described the disseminated form of pagetoid reticulosis in 19319,[10] in a 58-year-old man presenting with erythematous patches and nodules located primarily on the lumbar region, buttocks, and extensor surfaces of his arms and legs.[9] The diffuse disease is reported to have aggressive clinical behavior as opposed to the more indolent features of Woringer-Kolopp disease.[11] Cases reported under this entity, however, are heterogenous.
Woringer-Kolopp disease affects males twice as often as females, most commonly in middle-aged patients.[12] The most common presentation is a solitary, indolent, verrucous lesion on the distal extremities that commonly remains without a definitive diagnosis for several years.[13,14] The authors’ patient is a young woman who presented with a scaling erythematous plaque and a shorter clinical duration than typical for newly diagnosed Woringer-Kolopp disease, thus resulting in a smaller and flatter plaque.
Mycosis fungoides is characterized pathologically by a dense infiltrate of polymorphic atypical lymphocytes. The neoplastic lymphocytes are typically present in the epidermis. However, as the lesions progress from patch to plaque to tumor, the atypical cells extend into the dermis and can be present even in the subcutaneous fat.[15,16] The neoplastic cells show increased size, hyperchromatic nuclei, and a perinuclear halo.[17] Localized pagetoid reticulosis differs histologically from mycosis fungoides by increased hyperkeratosis and marked epidermotrophism of the atypical lymphocytes.[1,18]
The tumor cells of mycosis fungoides are invariably of a CD4+ phenotype.[19,20] The immunohistochemical analysis of the solitary plaques of pagetoid reticulosis has revealed several possible phenotypes, including CD4+, CD8+, or CD4-/CD8-.[19–22] These immunophenotypes appear to have no prognostic significance in Woringer-Kolopp disease.[9,23] CD8+ atypical lymphocyte-predominance, as seen in the authors’ patient, is observed in nearly half of the reported cases.[20,24]
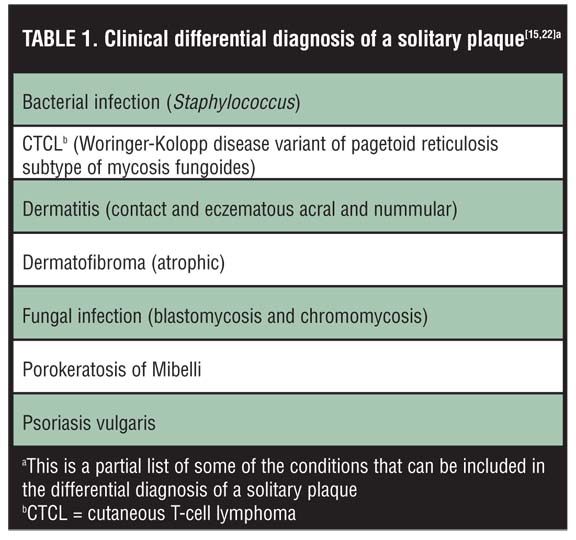
The clinical differential diagnosis of pagetoid reticulosis is broad due to the nonspecific morphology of a solitary, indolent plaque.22 Some of the conditions included in the differential diagnosis of a single cutaneous plaque are listed in Table 1. The diagnosis of pagetoid reticulosis is often delayed for several years because Woringer-Kolopp disease is an uncommon condition that is rarely suspected.[25] For example, pagetoid reticulosis was not initially considered as a diagnostic possibility in the patient in this case. Diagnoses of an atrophic dermatofibroma and porokeratosis were entertained. However, the clinical features of the lesion were unusual, thus prompting an early biopsy and histological analysis.
{kind=link}
Treatment options for localized pagetoid reticulosis include the following modalities: electron beam, pharmacological intervention, psoralen plus ultraviolet A (PUVA) photochemotherapy, radiotherapy, and surgery.[26,27] Electron beam, developed in the 1950s, is the oldest treatment for cutaneous T-cell lymphomas.[28] Nitrogen mustard is a commonly used pharmacological agent, but it is not universally effective.[22,28] Surgical excision was previously used when there were a few small and discrete lesions; however, the current excellent response of pagetoid reticulosis to topical and/or radiation therapy makes surgical intervention a treatment modality of perhaps historic significance.[3,22] The most effective treatment for severe Woringer-Kolopp disease is localized radiation therapy.[22] Newer topical therapies for cutaneous T-cell lymphomas, such as the retinoid receptor antagonist bexarotene, have not been explored as treatment for Woringer-Kolopp disease, but may prove to be a therapeutic option in the future.[28]
Conclusion
Pagetoid reticulosis can present as a solitary lesion or as a generalized disease. The authors describe a young woman with the localized form (Woringer-Kolopp disease) with CD8+ phenotype. Woringer-Kolopp disease is most commonly seen in middle-aged men as a solitary lesion on either the upper or lower extremities, and it should always be considered in the differential diagnosis when a patient presents with such a lesion.[12–14] A histological analysis reveals atypical lymphocytes primarily localized to the epidermis with a CD4+, CD8+, or CD4-/CD8- phenotype.[19,22] The treatment of choice for a solitary lesion may be localized radiation therapy, but the use of other therapies, such as bexarotene (gel or capsules), may warrant future investigation.[22,28]
References
1. Matsuzaki Y, Kimura K, Nakano H, Hanada K, Sawamura D. Localized pagetoid reticulosis (Woringer-Kolopp disease) in early childhood. J Am Acad Dermatol. 2009;61:120–123.
2. Miedler JD, Kristjansson AK, Gould J, Tamburro J, Gilliam AC. Pagetoid reticulosis in a 5-year-old boy. J Am Acad Dermatol. 2008;58:679–681.
3. Berroeta L, Lewis-Jones MS, Evans AT, Ibbotson SH. Woringer-Kolopp (localized pagetoid reticulosis) treated with topical photodynamic therapy (PDT). Clin Exp Dermatol. 2005;30:446–447.
4. Steffen C. Ketron-Goodman disease, Woringer-Kolopp disease, and pagetoid reticulosis. Am J Dermatopathol. 2005;27:68–85.
5. Cribier B. History: Frederic Woringer (1903-1964) and Woringer-Kolopp disease. Am J Dermatopathol. 2005;27: 534–545.
6. Skiljevic D, Bogdanovic Z, Vesic S, et al. Pagetoid reticulosis of Woringer-Kolopp. Dermatol Online J. 2008;15:18.
7. Woringer F, Kolopp P. Lesion erythemato-squameuse polycyclique de l’avant-bras evoluant depuis 6 ans chez un garconnet de 13 ans: histologiquement infiltrat-epidermique d’apparence tumorale. Ann Dermatol Syph. 1939;67: 945–958.
8. Braun-Falco O, Marghescu S, Wolff H. Pagetoide reticulose. Morbus Woringer-Kolopp. Hautarzt. 1973;24:11–21.
9. Pagnanelli G, Bianchi L, Cantonetti M, et al. Disseminated pagetoid reticulosis presenting as cytotoxic CD4/CD8 double negative cutaneous T-cell lymphoma. Acta Derm Venereol. 2002;82:314–316.
10. Ketron LW, Goodman MH. Multiple lesions of the skin apparently of epithelial origin resembling clinically mycoses fungoides. Arch Dermatol Syph. 1931;24:758–785.
11. Nakada T, Sueki H, Iijima M. Disseminated pagetoid reticulosis (Ketron-Goodman disease): six-year follow-up. J Am Acad Dermatol. 2002;47:183–186.
12. Mandojana RM, Helwig EB. Localized epidermotropic reticulosis (Woringer-Kolopp disease). J Am Acad Dermatol. 1983;8:813–829.
13. Lu D, Patel KA, Duvic M, Jones D. Clinical and pathological spectrum of CD8-positive cutaneous T-cell lymphomas. J Cutan Pathol. 2002;29:465–472.
14. Cerroni L, Fink-Puches R, El-Shabrawi-Caelen L, et al. Solitary skin lesions with histopathologic features of early mycosis fungoides. Am J Dermatopathol. 1999;21:518–524.
15. Jacyk WK, Grayson W, Dinkel JE, Requena L. Pagetoid reticulosis with CD30 positivity and cytotoxic/suppressor cells. J Cutan Pathol. 2007;34:644–647.
16. Zackheim HS. Is “localized epidermotropic reticulosis” (Woringer-Kolopp disease) benign? J Am Acad Dermatol. 1984;11:276–283.
17. Waitzer S, Fisher B. Woringer-Kolopp disease: a form of mycosis fungoides. Int J Dermatol. 1984;23:610–612.
18. Crowson AN, Magro CM. Woringer-Kolopp disease. A lymphomatoid hypersensitivity reaction. Am J Dermatopathol. 1994;16:542–548.
19. Gorpelioglu C, Sarifakioglu E, Haltas H. Spider bite-induced pagetoid reticulosis. J Eur Acad Dermatol Venereol. 2009;23:446–447.
20. Burns MK, Chan LS, Cooper KD. Woringer-Kolopp disease (localized pagetoid reticulosis) or unilesional mycosis fungoides? An analysis of eight cases with benign disease. Arch Dermatol. 1995;131:325–329.
21. Sedghizadeh PP, Allen CM, Kalmar JR, Magro CM. Pagetoid reticulosis: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:318–323.
22. Lee J, Viakhireva N, Cesca C, et al. Clinicopathologic features and treatment outcomes in Woringer-Kolopp disease. J Am Acad Dermatol. 2008;59:706–712.
23. Mourtzinos N, Puri P, Wang G, Liu M. CD4/CD8 double negative pagetoid reticulosis: a case report and literature review. J Cutan Pathol. 2010;37:491–496.
24. Palmer RA, Keefe M, Slater D, Whittaker SJ. Case 4: Pagetoid reticulosis (Woringer-Kolopp type) or unilesional mycosis fungoides (MF). Clin Exp Dermatol. 2002;27:345–346.
25. Lichte V, Ghoreschi K, Metzler G, et al. Pagetoid reticulosis (Woringer-Kolopp disease). J Dtsch Dermatol Ges. 2009;7:353–354.
26. Haghighi B, Smoller BR, LeBoit PE, et al. Pagetoid reticulosis (Woringer-Kolopp disease): an immunophenotypic, molecular, and clinicopathologic study. Mod Pathol. 2000;13:502–510.
27. Howard MS, Smoller BR. Mycosis fungoides: classic disease and variant presentations. Sem Cutan Med Surg. 2000;19: 91–99.
28. Duvic M. Current treatment of cutaneous T-cell lymphoma. Dermatol Online J. 2001;7:3.