
James Q. Del Rosso, DO, FAOCD
Introduction
The solid phase porous microsphere (hereafter referred to as “microsphere”) is a vehicle technology comprising inert, porous, polymer, spherical microparticles designed to entrap active ingredient, allowing for a slower rate of delivery into skin.[1] Microsphere particles are also referred to as microsphere beads or microsponges. The chemical manufacture of microspheres involves careful polymerization using specific inert monomers, which may be selected based on their compatibility with individual active ingredients. The method of microsphere manufacture is dependent on the chemical characteristics and “fragility” of the active ingredient. In the case of tretinoin, which is subject to being degraded by the polymerization process, the microspheres are produced first followed by subsequent “loading” of the active ingredient into the preformed microsphere beads.[1] In other cases, the active ingredient can be incorporated into the microspheres during the polymerization process without degradation of the active agent.
This article addresses clinically relevant considerations related to the microsphere vehicle system and specifically reviews data related to benzoyl peroxide (BP) microsphere formulations.
What features of microsphere vehicle technology are clinically relevant to dermatologic practice?
Recognizing that microspheres differ from other commonly used vehicle technologies, especially liposomes, is important. Liposomes are lipid bilayers that enclose drug molecules and can fuse with the lipid bilayer of the intercellular lipid membrane of the stratum corneum. Liposomal drug delivery may allow for improved cutaneous delivery of some active ingredients.[1] Use of liposomes in topical formulations is limited by the high potential for chemical instability, difficulty with the incorporation of some active ingredients, and expense.[1]
A potential advantage of microsphere technology is that epidermal delivery is targeted, correlated with a lower potential for transdermal penetration and systemic exposure.[1] As the active ingredient is “housed” within the microsphere particle, its slow release avoids an epidermal “overload” of active drug. Progressive topical delivery of the active ingredient into the epidermis may occur without rapid production of a drug concentration gradient, which serves to drive transcutaneous penetration into the systemic circulation.[1]
Additionally, the reduced cutaneous penetration rate of active ingredient associated with the microsphere vehicle appears to improve skin tolerability, at least with some active ingredients.[1–4] Formulations that are designed to optimize percutaneous penetration of active ingredient into skin often contain “penetration enhancers,” such as high concentrations of propylene glycol or dimethyl sulfoxide (DMSO), both of which may be associated with an increased risk of adverse events.[1,5] Microspheres avoid the rapid rise in epidermal concentration of active ingredient, which reduces cutaneous irritation with some agents, especially when the irritation potential is concentration-dependent.
Microsphere size is important with regard to cosmetic elegance of the final product. If the microsphere particle size is ?200 microns, the product is likely to exhibit a grainy or rough feel on application.[1] Currently available commercial products utilize microspheres with a particle size range of 5 to 50µm, which are not palpable on application. Although most users of microsphere formulations find them easy to apply and inconspicuous, occasionally patients report a fine white powder after drying, which has been noted to be beneficial in reducing “facial shine” and perception of skin oiliness in patients with acne.[6] Microspheres have been shown to produce greater oil (sebum) absorbance (w/w) as compared to conventional compounds used in cosmetic products, such as talc, kaolin, bentonite 670, and corn starch.[7]
Once the microsphere is formed with the incorporation of the active ingredient, the final formulation is stable at extremes of pH and heat (up to 130ºC).[1] The microsphere particles provide a reservoir, which alters pharmacokinetic delivery of the active ingredient by producing essentially two phases of drug gradient. After application of the microsphere vehicle to skin, as the active ingredient is slowly released from its entrapped state, it reaches steady-state with the vehicle phase of the formulation and ultimately with the epidermis. With active ingredients of moderate solubility in the vehicle phase, there is continued entrapment of the active agent as the epidermis is progressively exposed to steadier drug delivery.[7] Ultimately, when the active ingredient, micrsosphere design, and the remaining vehicle phase of the formulation are properly integrated, the final result is a formulation that is capable of percutaneous delivery of the active ingredient with a lower potential for cutaneous irritation.
When present within the microsphere, the active ingredient is somewhat protected from potential chemical reactivity or degradation by other external contactants or environmental exposures, such as ultraviolet (UV) light (sunlight).1 Active ingredients that are not highly compatible, such as hydroquinone and retinol, may be “separated” until the time of application to skin. Agents that are sensitive to UV light, such as tretinoin, are significantly protected from degradation while entrapped within the microsphere particles.[8]
What commercially available topical agents incorporate microsphere vehicle technology?
Several different ingredients can be incorporated into microspheres.[1] At present, commercially available, over-the-counter formulations using microsphere vehicles incorporate facial moisturizers, some cosmeceutical “skin rejuvenation” agents, and sunscreens. Prescription topical agents using microsphere vehicles include tretinoin microsphere gel 0.1% and 0.04% (Retin A Micro, OrthoNeutrogena, Skillman, New Jersey), BP microsphere cream 5.5% (NeoBenz Micro in tube and single-dispense delivery systems, SkinMedica, Inc., Carlsbad, California), BP microsphere wash 7% (NeoBenz Micro Wash Plus Pack, SkinMedica, Inc.), 5-fluorouracil cream 0.05% (Carac, Dermik, Bridgewater, New Jersey), and hydroquinone 4% with retinol cream (EpiQuin Micro, SkinMedica, Inc.).
What is the rationale behind the incorporation of BP into the microsphere cream?
From a microbiological perspective, BP is a vital component of acne therapy, exhibiting marked suppression of Propionibacterium acnes and reduced proliferation and emergence of antibiotic-resistant P. acnes strains with both “leave on” and wash formulations.[9,10] BP is not associated with resistance to its own antimicrobial properties.[9,10] Multiple studies have confirmed the therapeutic benefit of BP, both alone and in combination with other agents, such as topical antibiotics and topical retinoids.[11–14] In fact, BP is considered to be an integral component of first-line therapy for acne vulgaris, based on its ability to markedly reduce inflammatory acne lesions and its ability to moderately reduce comedonal acne lesions.[9,11] BP may also be used successfully as a component of long-term maintenance therapy.[11] Other than the potential for cutaneous irritation in some patients, which appears to be both concentration-dependent and vehicle-dependent, there are no major cutaneous or systemic safety concerns with application of BP, which has been used extensively for approximately five decades.[9]
The incorporation of BP into microsphere particles within a cream base involved the evaluation of the release characteristic of BP using Franz diffusion cell assays, which confirmed biphasic release of BP.1 This information confirmed that BP could be housed with the microsphere beads with slow progressive release. With BP, this finding is clinically relevant as the potential for irritation with BP is concentration-dependent, and as BP is converted within hours to benzoic acid, slower and more progressive delivery of BP into skin may produce more sustained therapeutic activity.[1,9] Irritancy studies using both animal and human skin models demonstrated a reduced potential for cutaneous irritation with BP in the microsphere vehicle.[1]
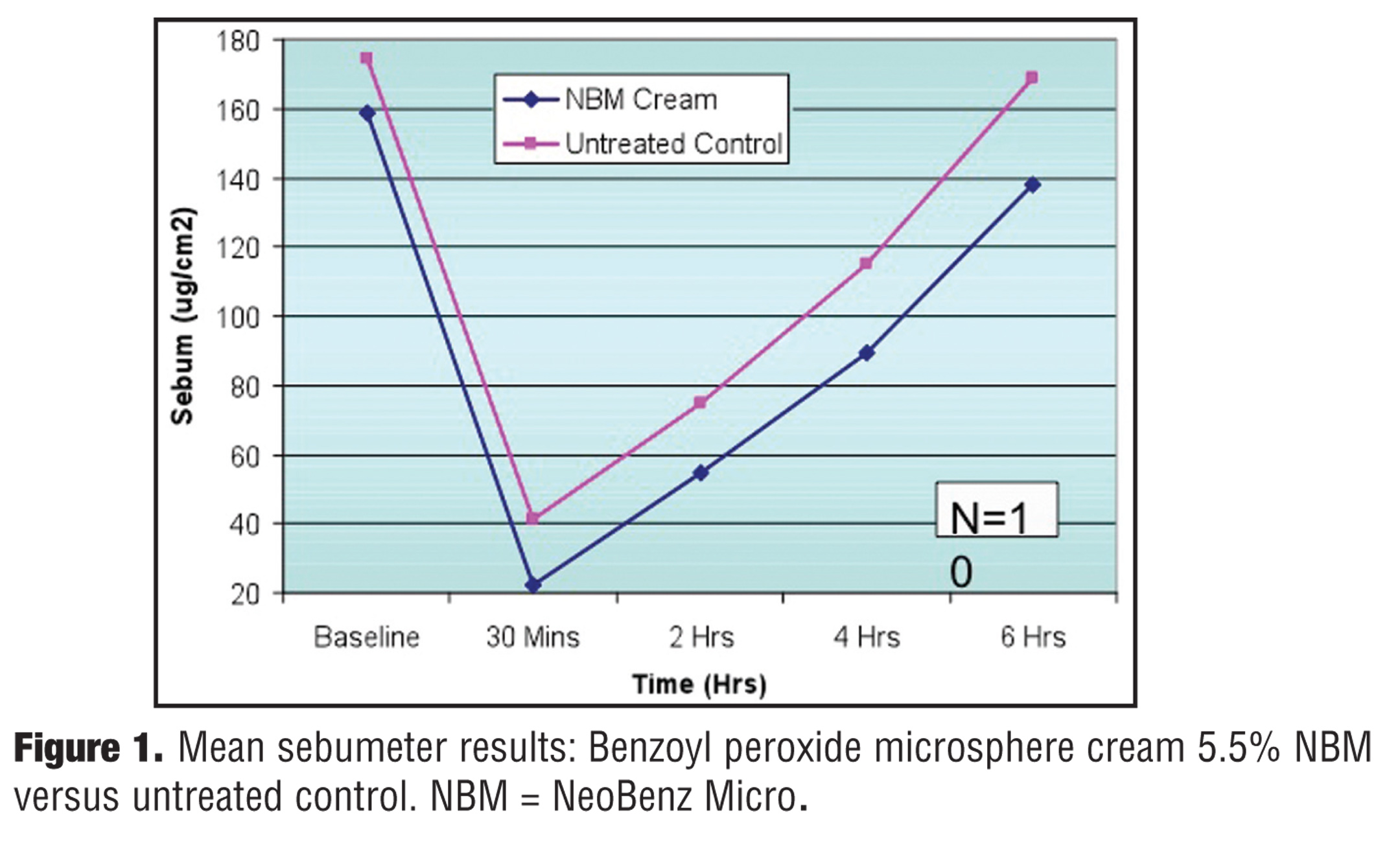
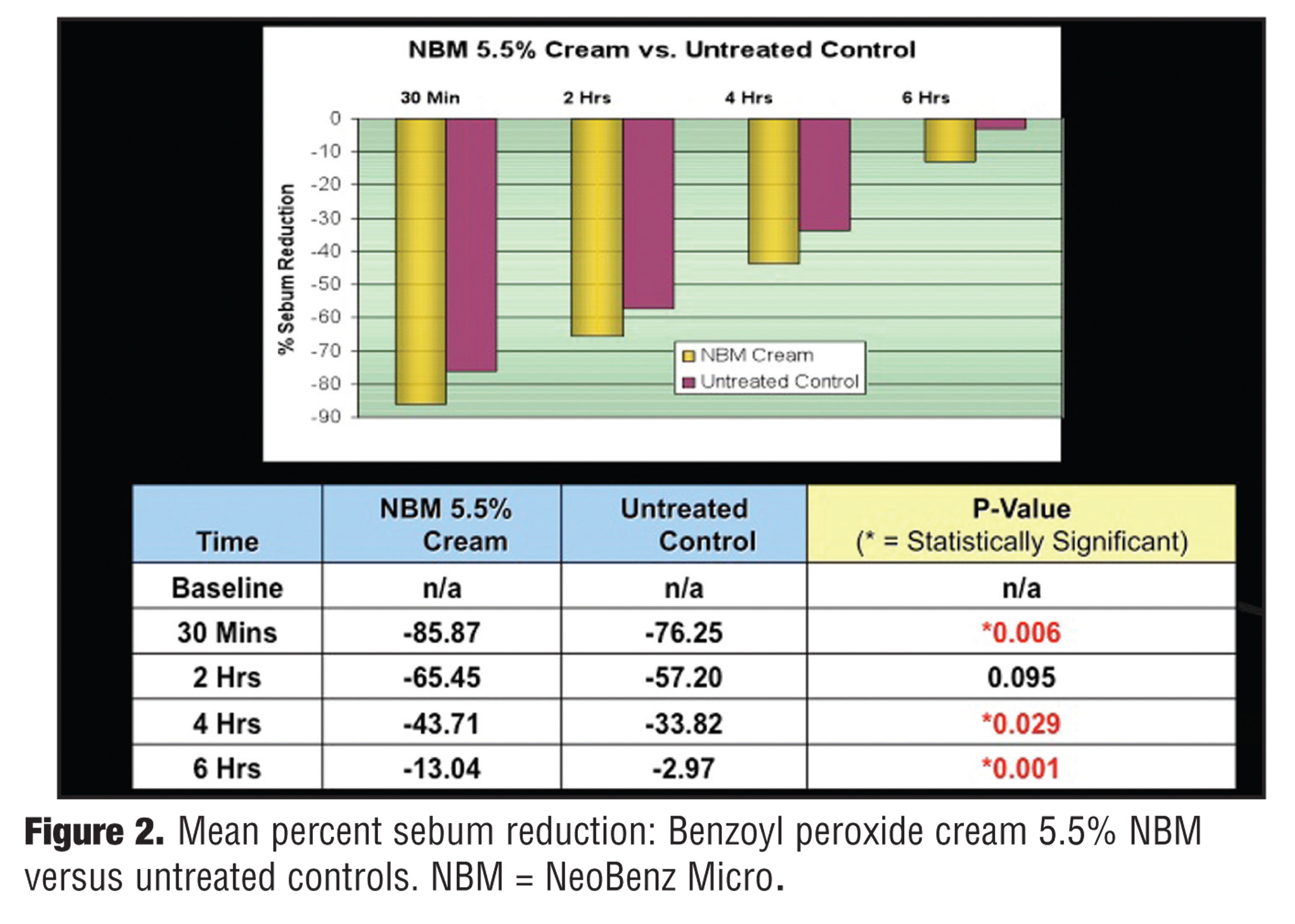
As discussed above, microspheres have also been reported to reduce “facial shine” and perception of skin oiliness in patients with acne, likely related to absorbance of sebum by the microsphere particles.[6] In a split-face study of subjects with “oily skin” (N=10), assessment of sebum reduction was measured over six hours on the forehead after cleansing with a designated gentle liquid cleanser and application of BP microsphere cream 5.5% on one side (active treatment side) versus after cleansing with a designated gentle liquid cleanser alone on the other side (untreated control side).[15] A sebumeter was used to measure sebum at baseline, 30 minutes, two hours, four hours, and six hours on both sides of the forehead. Results demonstrated greater sebum reduction on the actively treated sides with sebum measurements and mean percent sebum reductions depicted in Figure 1 and Figure 2, respectively.
{kind=link}
{kind=link}
The commercially available microsphere particle used for incorporation into the cream vehicle is patented under the designation of Microsponge®. After successful completion of the polymerization and active ingredient incorporation process with BP into microspheres and proof of reservoir capability and reduced irritancy using in-vitro skin models, the next step was to test the BP microsphere cream in patients with acne vulgaris in a controlled clinical trial.
What clinical data is available on BP microsphere cream in acne vulgaris?
In an investigator-blinded, randomized, multicenter, 12-week study, subjects ?12 years of age (N=48) with mild-to-moderate facial acne vulgaris were treated with either BP microsphere cream 5.5% twice daily or BP gel 6% twice daily.[16] The mean age of enrolled subjects was 17.1 years (range 12–37 years), with 26 males and 22 females included. Forty-three subjects were Caucasian, four were African American, and one reported being a mixture of Caucasian and African American. Conventionally recognized inclusion and exclusion criteria used in acne studies were incorporated into the study protocol, including appropriate washout periods for previously used acne medications, and exclusion of other therapies that may influence outcomes during the course of the trial, such as medications and physical modalities (e.g., facial peels, light therapies, and laser treatments).
The mean inflammatory, noninflammatory, and total lesion counts at baseline in the BP microsphere cream 5.5% were 26.3, 36.2, and 62.5, respectively and in the BP gel 6% group were 29.8, 44.7, and 74.4, respectively.[16] All subjects were evaluated for efficacy and safety, including assessment of application-site tolerability. Efficacy parameters included mean percent change in inflammatory, noninflammatory, and total acne lesions; change in acne severity scores (6-point scale); investigator global assessment of improvement (5-point scale); and subject global assessment of improvement (5-point scale). The six-point scale for static grading of acne severity was based on overall visible assessment by the investigator of the number or predominance of inflammatory and noninflammatory acne lesions. The five-point scale used for investigator and subject global assessments as compared to baseline ranged from a grade of 0, which indicated no improvement or worsening, to 4, which correlated with complete clearance. Facial skin-tolerability assessments were completed using a four-point scale by the investigator for erythema, dryness, and scaling, and by the subject for stinging and burning. The four-point tolerability scale ranged from 0, which correlated with none, to 3, which correlated with severe. Subject ratings of overall satisfaction with treatment were also documented.
By Week 4, both the BP microsphere cream 5.5% and BP gel 6% groups demonstrated statistically significant mean percent reductions in inflammatory and total lesions (P<0.05) as compared to baseline.16 In the BP microsphere cream 5.5% study arm, the mean percent reduction in inflammatory and total acne lesions at Week 4 were 40 percent and 30 percent, respectively. In the BP gel 6% study group, the mean percent reduction in inflammatory and total acne lesions at Week 4 were 26 percent and 12 percent, respectively. The mean percent reduction in noninflammatory lesions was 22 percent in the BP microsphere cream 5.5% group and one percent in the BP gel 6% group.
At Week 12, in the BP microsphere cream 5.5% group, the mean percent reduction in inflammatory, noninflammatory, and total acne lesions was 39, 34, and 35 percent, respectively. In the BP gel 6% study group, the mean percent reduction in inflammatory, noninflammatory, and total acne lesions at Week 12 was 25, 19, and 21 percent, respectively. Although BP microsphere cream 5.5% outperformed BP gel 6% based on mean percent reduction of inflammatory, noninflammatory, and total acne lesions at both Week 4 and Week 12, the differences in mean percent lesion reduction between the groups did not reach statistical significance at either follow-up time point with any of the acne lesion types, likely due to the small study population size.[16]
Differences in acne severity scores at Weeks 4 and 12 were observed between the two study groups.[15] In the BP microsphere cream 5.5% group, 67 percent and 48 percent of subjects demonstrated at least a one-grade improvement at Weeks 4 and 12, respectively; six percent and 19 percent of subjects demonstrated at least a two-grade improvement at Weeks 4 and 12, respectively.[16] In the BP gel 6% study arm, 31 percent and 42 percent of subjects demonstrated at least a one-grade improvement at Weeks 4 and 12, respectively; zero percent and five percent of subjects demonstrated at least a two-grade improvement at Weeks 4 and 12, respectively.
Overall, including both study groups, approximately 75 percent of subjects demonstrated at least some improvement of their acne based on investigator global assessments.[16] Complete clearance or marked improvement of acne was observed by the investigators in 33 percent of subjects treated with BP microsphere cream 5.5% and 16 percent of subjects treated with BP gel 6%. Approximately 90 percent of subjects demonstrated at least some improvement of their acne based on subject global assessments overall in both study groups. Marked improvement or better was noted by the subjects in 38 percent of those treated with BP microsphere cream 5.5% and 32 percent of subjects treated with BP gel 6%. Subject ratings of overall satisfaction with treatment were reported to be excellent or good in 67 percent of those treated with BP microsphere cream 5.5% and 68 percent of those treated with BP gel 6%, with more subjects treated with BP microsphere cream 5.5% rating their improvement as excellent (38% vs. 11%).
In a case report series of patients with acne vulgaris evaluating the use of BP microsphere cream (3.5%, 5.5%, or 8.5%) in combination with other agents, including topical retinoids, favorable therapeutic and cutaneous tolerability outcomes were observed.[14] Of note was a marked preference for the single dose (SD) sponge applicator, allowing for ease of application and portability when traveling as compared to a tube.
What clinical information is available on the skin tolerability of the BP microsphere cream?
In the investigator-blinded, randomized, multicenter, 12-week trial comparing BP microsphere cream 5.5% and BP gel 6%, signs of cutaneous irritation were assessed by the investigator, and symptoms of facial stinging and burning were reported by the subject.[16] Of the 48 subjects enrolled, only one subject withdrew from the trial, experiencing marked facial skin irritation after four days of application of BP gel 6%. Forty-six adverse events were reported among the 48 subjects, with more than one event reported in some subjects. The reported adverse events related primarily to facial skin tolerability reactions, including stinging, itching, scaling, dryness, and erythema. Almost all skin tolerability reactions were rated as mild, with most clearing and the remainder improving over the 12-week course of the study. In the BP gel 6% group, the overall incidence of facial skin tolerability reactions was 79 percent, including stinging (22%), itching (26%), scaling (9%), dryness (13%), and erythema (9%). In the BP microsphere cream 5.5% group, the overall incidence of facial skin tolerability reactions was 37 percent, including stinging (4%), scaling (29%), and dryness (4%).
What information is available on BP microsphere wash?
Data evaluating the prescription patterns of dermatologists collected over a five-year period (2001–2006) show that approximately 50 percent of BP prescriptions are for wash/cleanser formulations (hereafter referred to as “wash”).[17–20] Studies evaluating efficacy and safety of some BP washes have reported a decrease in P. acnes including antibiotic-resistant strains, reductions in both inflammatory and noninflammatory acne lesions, favorable skin tolerability, and ease of use with high adaptability for utilization on the face and trunk.[10,17–20] As approximately 50 percent of patients presenting with facial acne vulgaris also exhibit truncal acne vulgaris, addressing therapy for both the face and trunk is clinically relevant.[21] Importantly, 25 percent of patients who are seen for facial acne vulgaris yet also exhibit truncal involvement do not voluntarily mention the presence of acne lesions on their trunk.[21] However, more than 70 percent of these patients also desire treatment for their truncal acne vulgaris. As BP is known to bleach colored fabric, washes are generally favored over “leave on” vehicles when treating truncal acne vulgaris.[17–20]
A BP microsphere wash 7% was developed with the goal of creating a formulation that would provide efficacy while at the same time deliver both a very low level of cutaneous irritation and a high level of patient satisfaction. The microsphere particle used in the BP microsphere wash uses the same microsphere technology as the BP microsphere cream (Microsponge®).
Substantivity of the microsponge particles incorporated into the BP microsphere formulation has been demonstrated after completion of the prescribed lathering, rinsing, and patting dry.[15] Substantivity is defined as the adherence capability of a topical drug or cosmetic after skin is exposed to water or perspiration. Utilizing in-vivo confocal microscopy after the lathering, rinsing, and drying procedure, BP microspheres were visualized on the skin surface localized to perifollicular regions on the face.
What clinical information is available on BP microsphere wash?
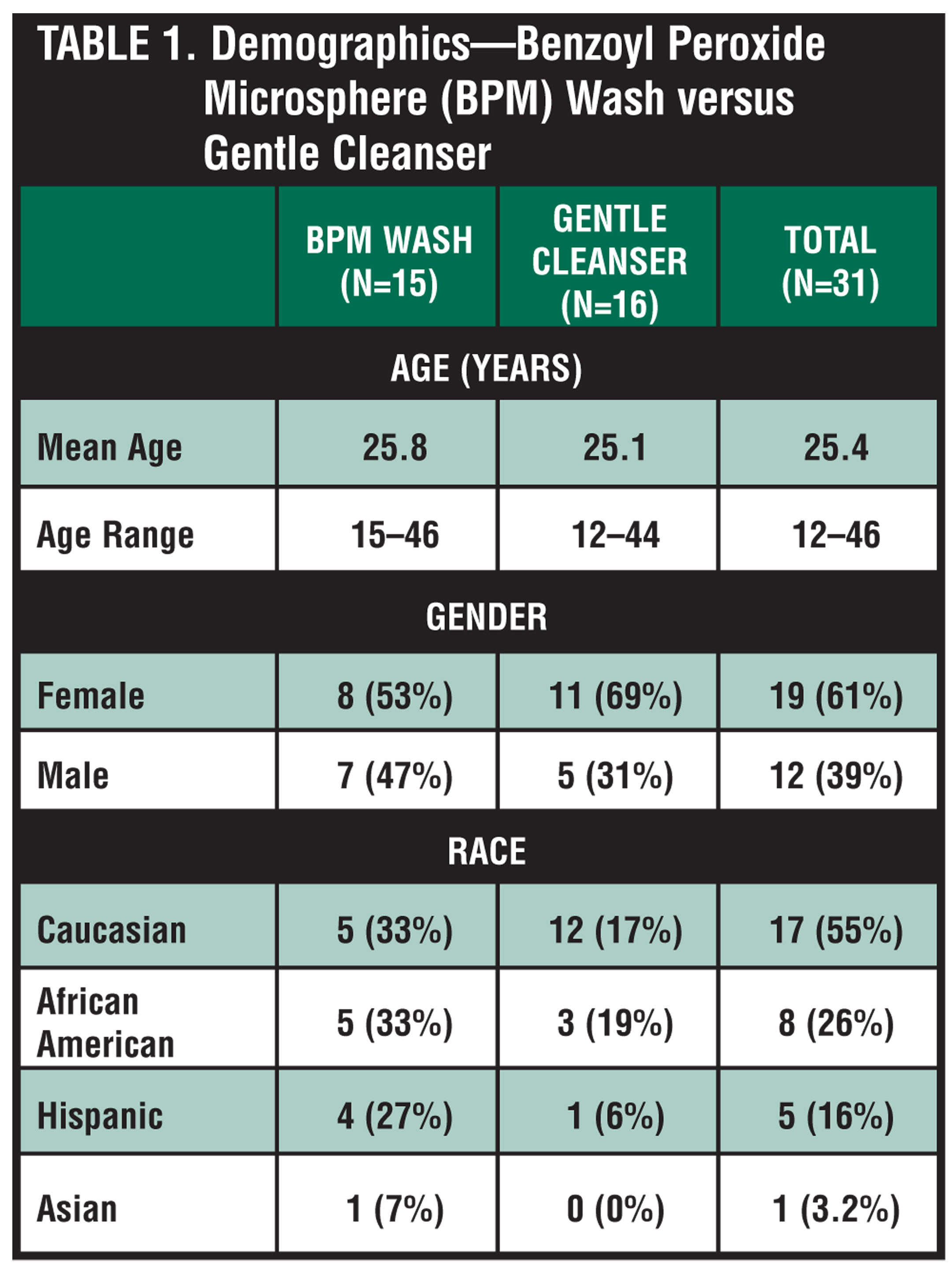
A multicenter, investigator-blinded, randomized, parallel group, three-week study compared skin tolerability of BP microsphere wash 5.5% once daily (n=15) versus a gentle nonmedicated cleanser once daily (n=16) in subjects ?12 years of age with facial acne vulgaris.[22] All subjects were also treated with clindamycin phosphate 1.2%/tretinoin 0.025% combination gel (clin/tret gel) once daily. Grading of acne severity for study inclusion was based on investigator global assessment using a standardized six-point scale, with 52 percent rated as mild severity and 48 percent rated as moderate severity at Baseline. Conventional exclusion criteria for acne study enrollment were employed including disallowance of any concomitant medications that could influence results, such as topical acne medications or other medications or physical modalities that could affect study outcomes. Additionally, all subjects had to report a history of using a stable skin care regimen for two weeks prior to enrollment. The study demographics are depicted in Table 1. No significant differences were noted between the two study groups in baseline characteristics, signs, or symptoms.
{kind=link}
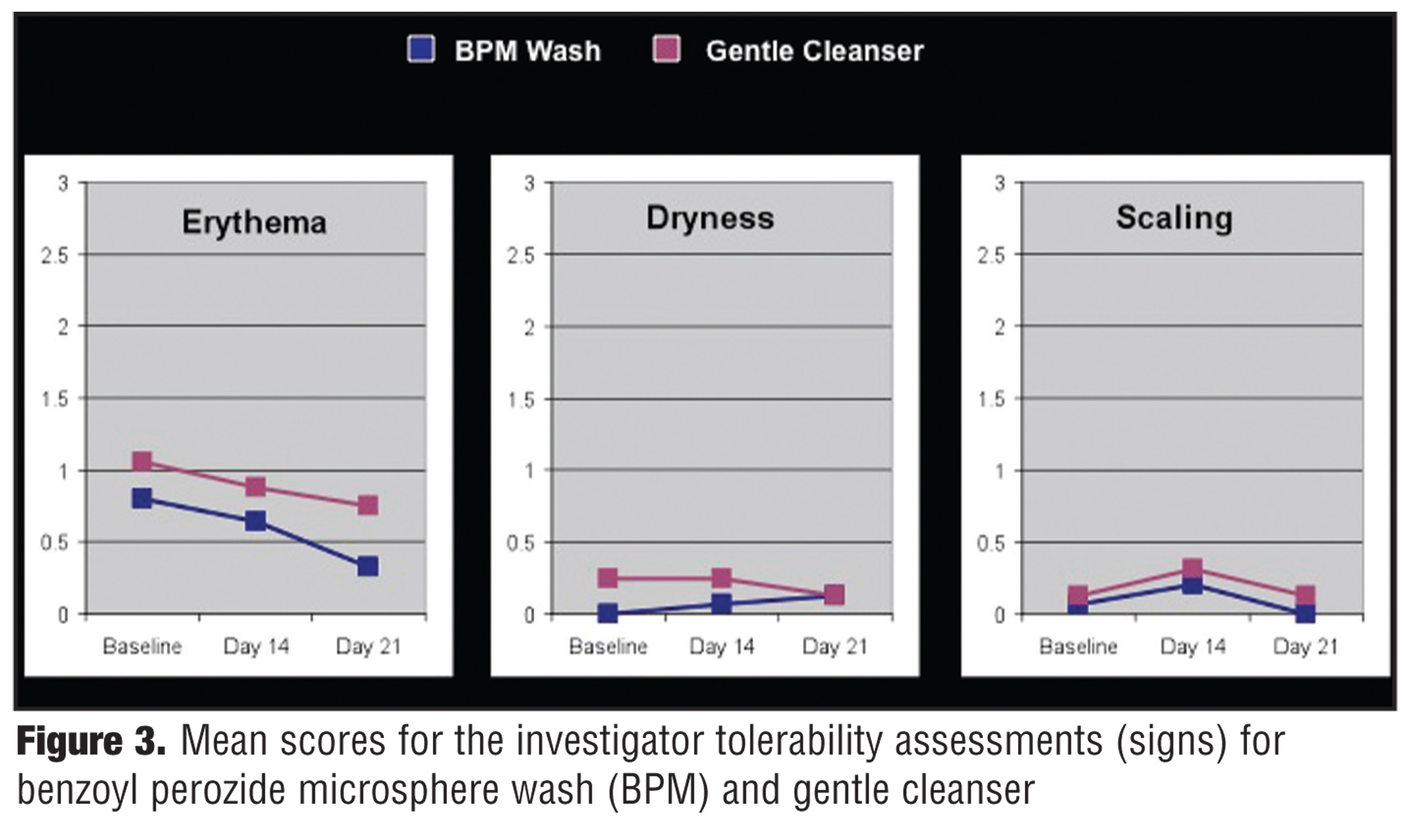
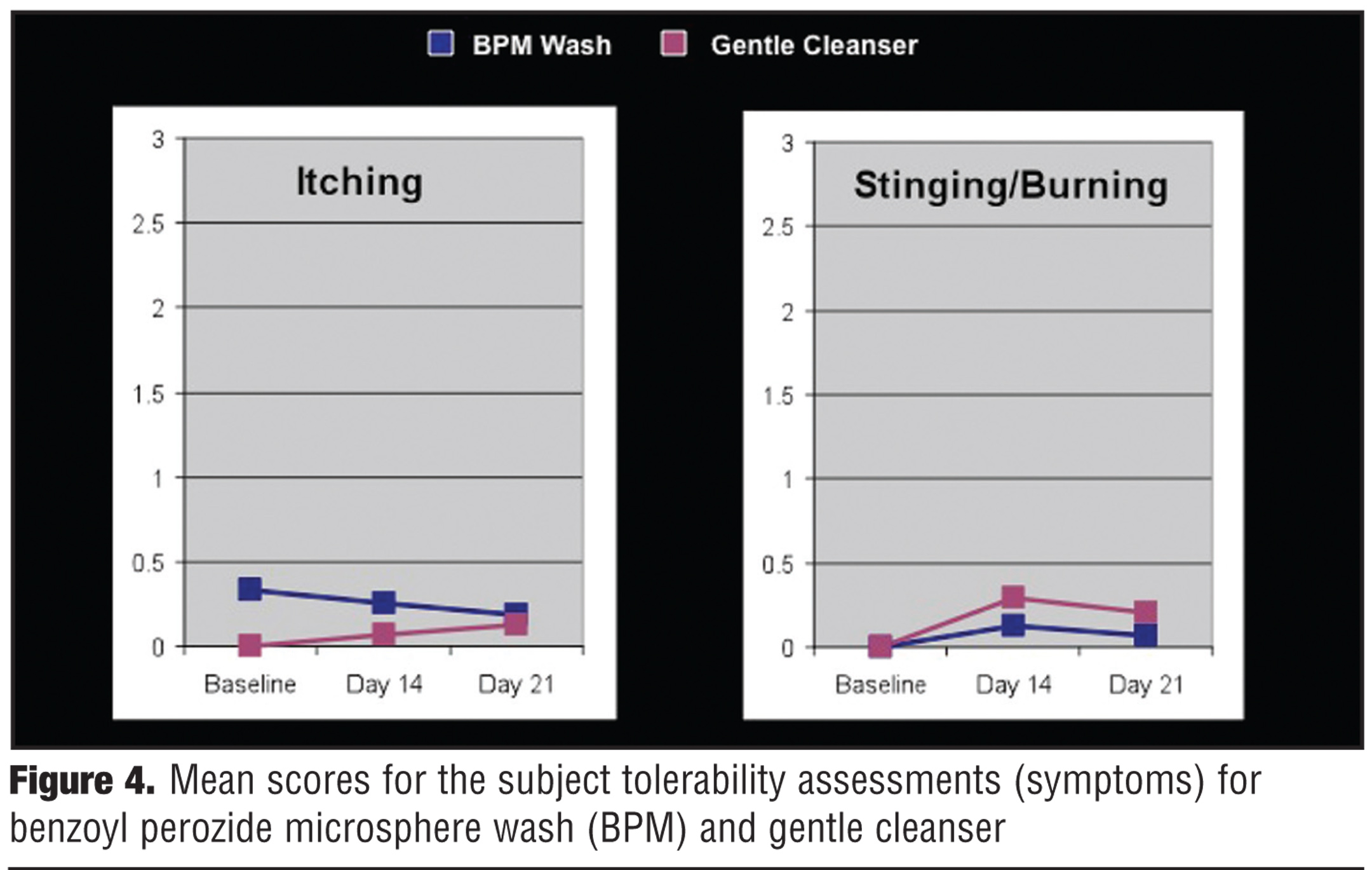
Tolerability assessments were completed using a four-point scale (0=none, 1=mild, 2=moderate, 3=severe).[22] The investigators evaluated signs of cutaneous irritation, such as erythema, dryness, and scaling. The subjects reported any symptoms associated with cutaneous irritation, such as itching and stinging/burning. Evaluations were completed at Baseline, Day 14, and Day 21. At Day 21, subjects also completed a questionnaire related to their perceptions of the aesthetic attributes of the product they used and satisfaction with the therapeutic regimen.
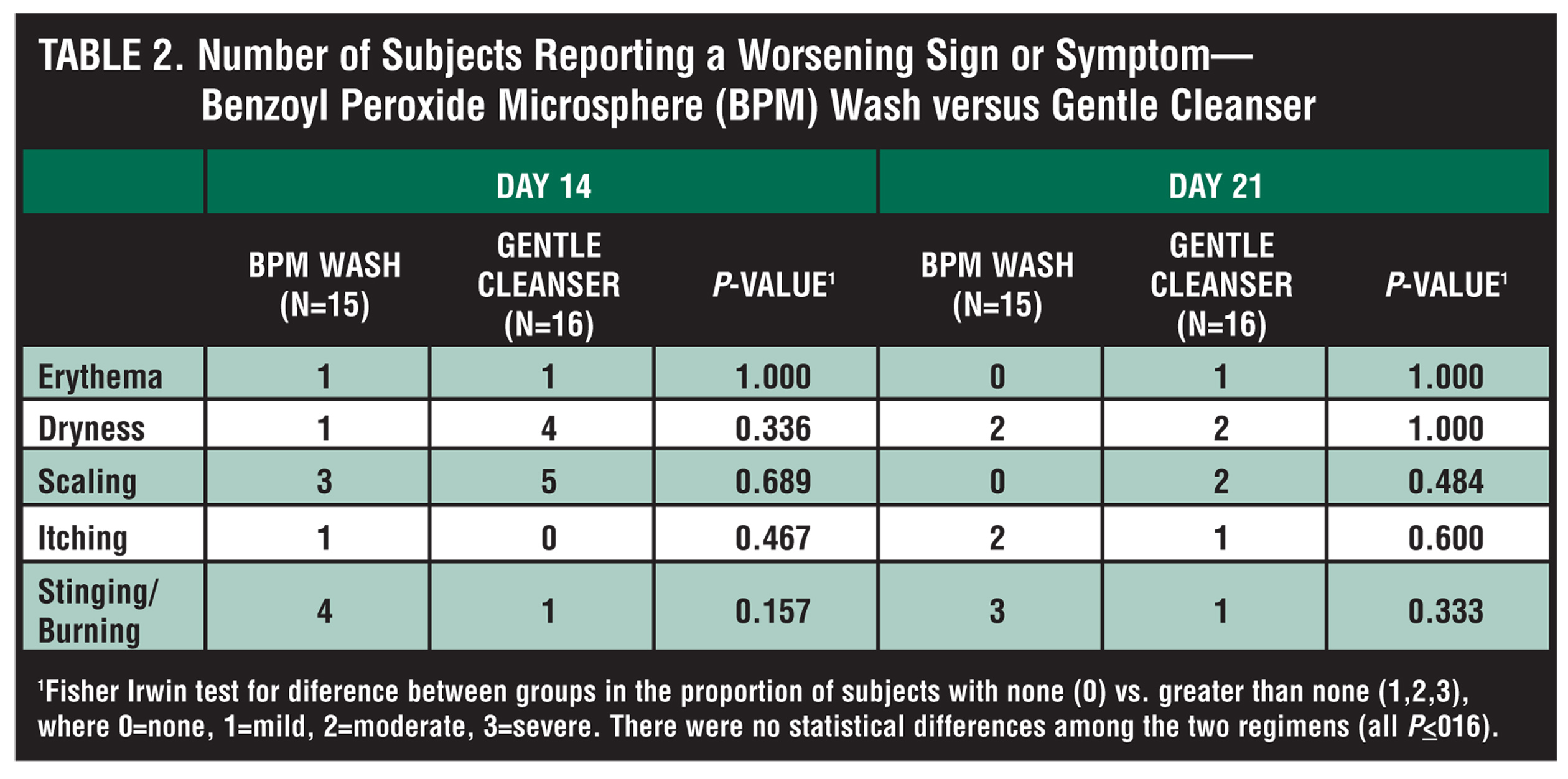
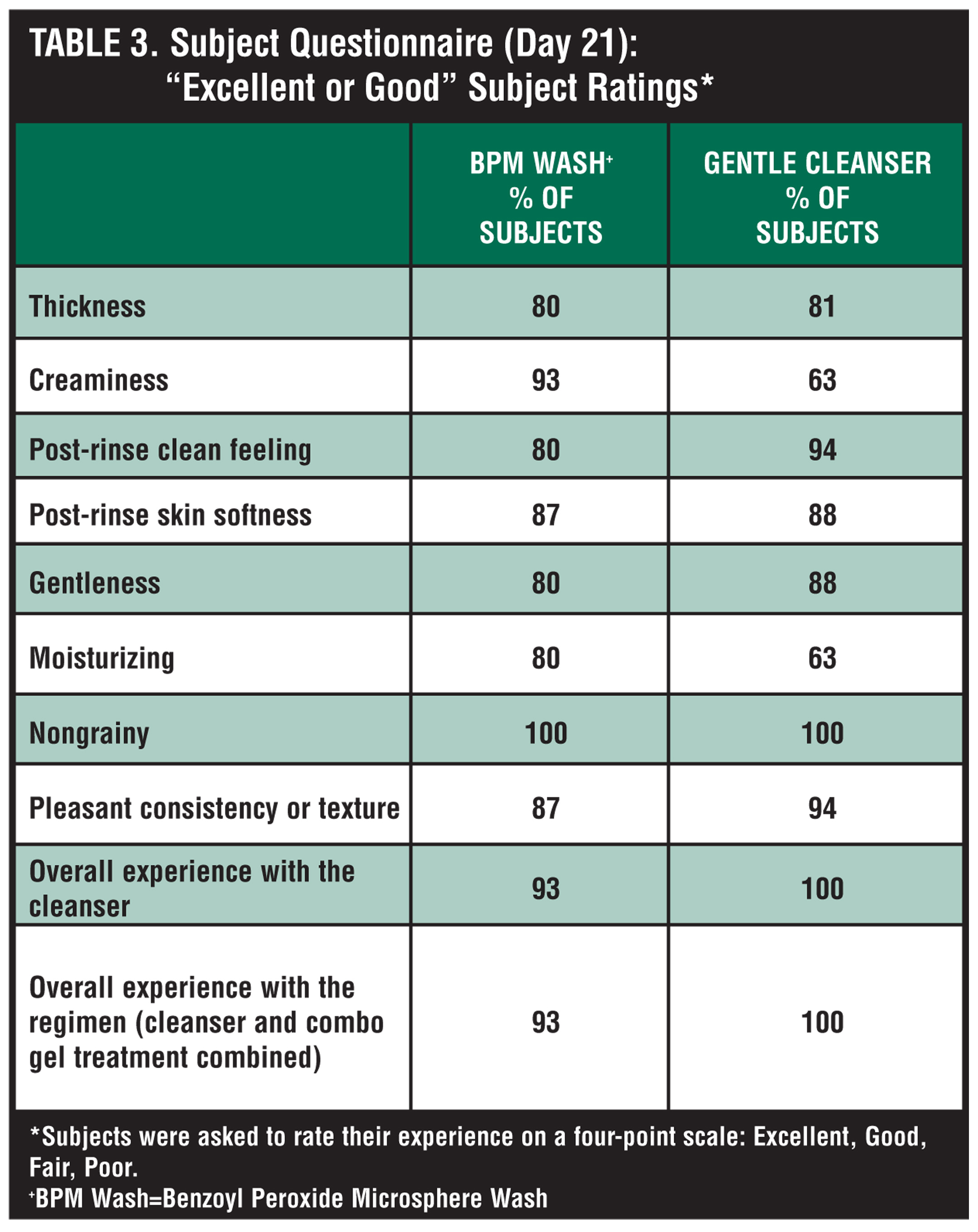
Figure 3 graphically shows investigator evaluation results for mean scores for signs related to facial skin tolerability. Mean scores for reporting of symptoms by subjects related to facial skin tolerability are depicted in Figure 4. Table 2 shows the number of subjects reporting a worsening of a sign or symptom related to facial skin tolerability. Based on both investigator and subject evaluations, both study groups exhibited low mean tolerability scores (?0.3) for dryness, scaling, itching, and stinging/burning. Interestingly, in both study groups, the baseline median erythema score was “1.” However, in the BP microsphere wash group, the median erythema score decreased to “0” by end of study (Day 21). Table 3 depicts the results of the questionnaire completed at the end of the study noting the subject ratings of “excellent” or “good” for each question. Overall, the results of this study demonstrated that the BP microsphere wash used in combination with clin/tret gel once daily was equally as tolerable as the use of a gentle nonmedicated cleanser along with clin/tret gel once daily. Both regimens were associated with a highly favorable skin-tolerability profile. Additionally, subjects reported very high ratings of the aesthetic qualities and satisfaction with treatment using the BP microsphere wash. From a patient adherence perspective, the therapeutic regimen employed in this study is “patient friendly” in terms of convenience, as there is a single “wash step,” which is also the same single single “product application” step. Convenience of use, favorable skin tolerability, and aesthetic acceptance of the products used are likely to improve adherence with treatment, although adherence was not formally measured as an endpoint in this study.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
As a BP wash is adaptable for treatment of both facial and truncal acne vulgaris, it was decided to increase the strength of the BP microsphere wash to 7%. This concentration was felt to be appropriate for use on both the face and the trunk, as most studies evaluating the use of a BP wash for truncal acne have incorporated BP in the higher concentration range (>6%).[17–19] The next step was to evaluate whether or not an increase in concentration to 7% would maintain the favorable tolerability profile that was demonstrated with this microsphere wash formulation.
In a single-center, randomized, investigator-blinded, three-week study, BP microsphere wash 7% once daily (n=23) was compared in terms of tolerability and preference to a gentle nonmedicated cleanser once daily (n=23) in subjects ?18 years of age with mild-to-moderate facial acne vulgaris.[23] Conventional exclusion criteria for acne study enrollment were employed and all subjects had to report a history of using a stable skin care regimen for four weeks prior to enrollment. Tolerability assessments were completed at Baseline and end of study (Day 21) using a four-point scale. The investigator assessed signs of cutaneous irritation (erythema, dryness/scaling), and the subjects noted symptoms related to facial skin tolerability (itching, stinging/burning). At end of study, subjects in both groups completed a questionnaire related to their perceptions of satisfaction and aesthetic attributes with the product they used.
Study results demonstrated that there were no statistically significant differences between the two study groups in objective (investigator) tolerability assessments, subjective (subject) tolerability assessments, or subject ratings related to satisfaction and aesthetic qualities with the used product.[23] An “excellent” or “good” rating for BP microsphere wash was reported by 87, 96, 83, and 100 percent of subjects for pleasant texture/consistency, creaminess, gentleness, and nongrainy texture, respectively. One-hundred percent of subjects stated that BP microsphere cream was “easy to use,” with 78 percent stating that they would continue to use it for acne treatment.
What conclusions can be made on microsphere vehicle technology and incorporation of BP into a microsphere cream vehicle?
Microsphere technology is an important advance in dermatology as it allows for progressive delivery of active ingredient into skin along with a favorable tolerability profile. Thus far, a variety of active ingredients have been incorporated into commercially available prescription and over-the-counter products using microspheres. Microspheres also provide physical and chemical stability for active ingredients and do not require a preservative to maintain microbiological stability. BP is available in both microsphere cream and microsphere wash formulations. Available studies demonstrate clinical relevance, especially related to high levels of skin tolerability, aesthetic attributes, and patient satisfaction.
References
1. Smith SS, Morhenn V, Webster G. Solid phase porous microspheres: a review. J Drugs Dermatol. 2006;5:969–976.
2. Summary basis of approval: Retin-A Micro 0.1%. www.accessdata. FDA.com. Accessed April 5, 2006.
3. Leyden JJ, Grove JL. Randomized facial tolerability studies comparing gel formulations of retinoids used to treat acne vulgaris. Cutis. 2001;67(suppl): 17–27.
4. Embil K, Nacht S. The microsponge delivery system (MDS): a topical delivery system with reduced irritancy incorporating multiple triggering mechanisms for the release of actives. J Microencapsul. 1996;13:575–588.
5. Smith EW, Surber C, Tassopoulos T, Maibach HI. Topical dermatological vehicles: a holistic approach. In: Bronaugh RL, Maibach HI, eds. Topical Absorption of Dermatological Products. New York: Marcel Dekker; 2002:457–463.
6. Nyirady J, Nighland M, Payonk G, et al. A comparative evaluation of tretinoin gel microsphere 0.1% versus tretinoin cream 0.025% in reducing facial shine. Cutis. 2000;63:153–156.
7. Saxena S, Nacht S. Polymeric porous delivery systems: polytrap and microsponge. In: Rosen MR, ed. Delivery System Handbook for Personal Care and Cosmetic Products Technology, Applications, and Formulations. Norwich, New York; William Andrew Publishing; 2005:333–350.
8. Nyirady J, Lucas C, Yusuf M, et al. The stability of tretinoin in tretinoin microsphere 0.1%. Cutis. 2002;70:295–298.
9. Tanghetti EA, Popp KF. A current review of topical benzoyl peroxide: new perspectives on formulation and utilization. Dermatol Clin. 2009;27:17–24.
10. Leyden JJ, Wortzman M, Baldwin EK. Antibiotic-resistant Propionibacterium acnes suppressed by a benzoyl peroxide cleanser 6%. Cutis. 2008;82:417–421.
11. Gollnick H, Cunliffe W, Berson D, et al. Management of acne: a report from a global alliance to improve outcomes in acne. J Am Acad Dermatol. 2003;49:S1–S38.
12. Del Rosso JQ. Study results of benzoyl peroxide 5%/clindamycin 1% topical gel, adapalene 0.1% gel, and use in combination for acne vulgaris. J Drugs Dermatol. 2007;6:616–622.
13. Tanghetti E, Abramovits W, Solomon B, et al. Tazarotene versus tazarotene plus clindamycin/benzoyl peroxide in the treatment of acne vulgaris: a multicenter, double-blind, randomized, parallel-group trial. J Drugs Dermatol. 2006;5:256–261.
14. Bikowski J, Del Rosso JQ. Benzoyl peroxide microsphere cream as monotherapy and combination treatment of acne. J Drugs Dermatol. 2008;7:590–595.
15. Data on file. SkinMedica, Carlsbad, California, 2009.
16. Smith SR, Kempers S. A study of 5.5% benzoyl peroxide microsphere cream versus 6% benzoyl peroxide gel in the treatment of acne vulgaris. Cosmet Dermatol. 2006;19:537–542.
17. Del Rosso JQ. What is the role of benzoyl peroxide cleansers in acne management? Do they decrease Propionibacterium acnes counts? Do they reduce acne lesions? J Clin Aesthetic Dermatol. 2008;1:48–51.
18. Del Rosso JQ. Benzoyl peroxide cleansers for the treatment of acne vulgaris: status report on available data. Cutis. 2008;82:336–342.
19. Leyden JJ, Del Rosso JQ, Webster GF. Clinical considerations in treatment of acne vulgaris and other inflammatory skin disorders: a status report. Dermatol Clin. 2009;27:1–15.
20. Gold M. Survey results of compliance, preference, and satisfaction in patients prescribed benzoyl peroxide 8% wash and benzoyl peroxide 9% cleanser for the treatment of acne vulgaris. Poster presented at American Academy of Dermatology Annual Meeting; March 2006; San Francisco, California.
21. Del Rosso JQ, Bikowski JB, Baum E, et al. A closer look at truncal acne vulgaris: prevalence, severity, and clinical significance. J Drugs Dermatol. 2007;6:597–600.
22. Del Rosso JQ, Kircik L. Comparison of the tolerability of benzoyl peroxide microsphere cream wash versus gentle cleanser when used in combination with clindamycin and tretinoin gel: a multicenter, investigator-blind, randomized study. Poster presented at: American Academy of Dermatology 67th Annual Meeting, March 6–10, 2009; San Francisco, California.
23. Trookman N, Rizer RL, Ho ET, Ford RO, Mehta RC. Randomized, evaluator-blinded, parallel group comparison study of the tolerability and subject preference of a benzoyl peroxide microsphere wash compared to a gentle non-medicated cleansing wash in mild to moderate acne. Poster presented at: American Academy of Dermatology Summer Meeting, July 30–August 2, 2009; Boston, Massachusetts.