
David K. Funt, MD, Assistant Clinical Professor, Plastic Surgery, Albert Einstein College of Medicine, Bronx, New York
Disclosure: Dr. Funt has received consulting fees for his work with Merz Aesthetics and serves as one of the company’s medical advisors. He is also part of the national speakers bureau of Allergan Corporation and receives honoraria for educational activities. Financial support for preparation of this manuscript was provided in part by Merz Aesthetics (San Mateo, California).
Abstract
As dermal fillers have evolved, volume restoration and contour enhancement have become the objective of advanced injectors. The value of injections of dermal fillers into the midface is well documented in the literature. However, the midface, particularly the infraorbital hollow, is the facial area most prone to adverse events from filler treatment. Malar edema is a particularly significant and long-lasting untoward event that is frequently reported. This article reviews the anatomic basis for malar edema, relates it to filler injection technique, and presents the author’s preferred method of injection to help ensure avoidance of this adverse event. (J Clin Aesthet Dermatol. 2011;4(12):32–36.)
The introduction of more durable and robust dermal filler materials has expanded the indications for dermal fillers, especially for the face. There probably is no area of the face that has not been treated with injectable fillers. Clinicians are now approaching facial aesthetic improvement and rejuvenation in a more global fashion, rather than focusing exclusively on the correction of wrinkles and folds. In contrast to amelioration of isolated wrinkles and folds, volume restoration and contour enhancement have become the objectives of advanced injectors. The value of midfacial volume restoration and enhancement has been well documented in the literature.[1–5] However, when treating this area, the injector can experience adverse events, including the significant and long-lasting complication of malar edema. This article presents the anatomic basis of malar edema and the author’s preferred injection technique to prevent this untoward event.
Midfacial Volume Restoration
The malar fat pad is a discrete, triangular shaped area of thickened subcutaneous fat, based at the nasolabial fold with its apex at the malar eminence in the youthful face. It is attached to the overlying skin and is supported by multiple fibrous septae that extend from the superficial musculoaponeurotic system (SMAS) and into the dermis. Loss of skin elasticity and weakening of these septae, as well as volume loss within the deep medial cheek fat,[6] lead to a downward and forward descent of the skin and malar fat pad until it bulges against the fixed nasolabial fold.
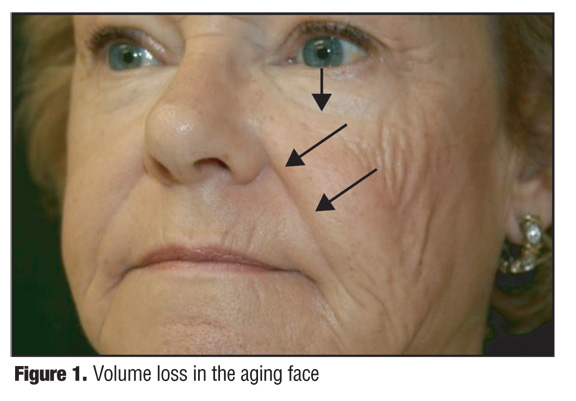
These sequelae of aging result in deepening of the nasolabial folds, progressive hollowing of the cheeks, and loss of prominence of the malar eminences. The lower eyelid lengthens, increasing visibility of the orbicularis oculi muscle, coupled with the formation of tear trough and a crescent or “V”-shaped deformity along the maxilla and zygoma. There is recession of the nasal alar cheek junction. Individual fat pockets become discernable as separate entities rather than the smooth transitions from convexities to concavities seen in youth (Figure 1). It is the author’s view that no other facial injection site provides greater rejuvenation than the midface.
{kind=link}
Fillers, alone or in conjunction with facial surgery, can restore facial harmony, balance, and beauty. Nevertheless, treatment of this area is not without its complications. Bruising, erythema, pain, infection, skin necrosis, over and under correction, and infraorbital nerve injury resulting in numbness and dysesthesia have been reported, regardless of the filler type (hyaluronic acid, calcium hydroxylapatite, poly-L-lactic acid) used. Nodules, lumps, visible material, and generalized and malar edema may also occur. Malar edema is a particularly significant adverse event because it is disfiguring, poorly tolerated by patients, can persist for months, and responds minimally, if at all, to treatment.
Anatomic Basis for Malar Edema
Malar edema is an adverse event arising from filler injections of the central midface to correct the infraorbital hollow and tear trough. It occurred in two patients treated by the author after placing calcium hydroxylapatite (CaHA, Radiesse®, Merz Aesthetics, San Mateo, California) in a retrograde linear threading and fanning technique from multiple access points. The edema was long lived—6 to 8 months—and only minimally responsive to massage, head elevation, taping, salt avoidance, methylprednisolone, and conservative intralesional steroid injections. Although these two cases involved CaHA, malar edema arising from injections with hyaluronic acid (HA) has also been seen in clinical practice.
The phenomenon of malar edema can be explained by an understanding of the anatomy of the lower eyelid. Pessa and Garza[6,7] reported their findings after performing 18 fresh cadaver dissections. Using dye injections, histological evaluation, and gross anatomical dissection, they identified a fascial structure of the lower eyelid and cheek that they called the malar septum. It originates from the orbital rim periosteum at the arcus marginalis superiorly and inserts into the cheek skin 2.5 to 3cm inferior to the lateral canthus. It divides the suborbicularis oculi fat (SOOF) into superior and inferior components. The inferior component is confluent with the cheek fat and the superior component contributes to the malar mounds. At the level of the inferior border of the orbicularis oculi, the malar septum fuses with the fibrous septa of the superficial cheek fat and dermis.
The authors stated that the malar septum is a relatively impermeable barrier that allows tissue edema and hemoglobin to accumulate superior to its cutaneous insertion, and thus defines the lower anatomical boundary of several clinical entities: malar edema, malar mounds, festoons, and periorbital ecchymosis. Its anatomy is consistent from person to person regardless of age.
Transcutaneous Preperiosteal Injection Using Limited Puncture Sites
The area bounded by the lower eyelid margin superiorly, the medial canthus medially, the lateral canthus laterally, and the submalar region inferiorly is the least forgiving and most prone to adverse events. Injected filler superficial to the malar septum may serve to augment the impermeable barrier of the malar septum, further impeding lymphatic drainage resulting in fluid accumulation and prolonged edema. Fillers may also cause edema by direct pressure on the lymphatics when volumes are too large whether they are superficial or deep to the septum. In addition, the greater a filler’s elasticity or elastic modulus (G’)—lifting capacity—the more likely it is to compress the lymphatic flow, resulting in edema. Malar edema is likely related to the volume of injectate, the filler’s physical characteristics, its depth of injection, and the patient’s propensity toward the problem.
Any filler injected within the boundaries of the malar septum should be placed immediately onto periosteum (preperiosteally). In addition to avoiding malar edema, placing small boluses of filler directly on bone has the additional advantage of avoiding lumps, nodules, and visible material. The result is more natural and aesthetically pleasing because it is an augmentation of the underlying skeletal structure, resulting in an expansion and elevation of the overlying soft tissue envelope. Since the material is placed in an avascular space, there is less bruising and lower embolic potential. Preperiosteal small bolus technique can be accomplished using either an intraoral or transcutaneous approach. The author prefers a transcutaneous approach because it is less technically demanding, easier to teach, has less risk of infraorbital nerve injury and in theory has less risk of infection and biofilm creation. Another approach would be the use of a nonparticulate, monophasic, less refractive HA capable of being placed in the subdermal plane without being visible or causing a Tyndall effect. This would allow correction of the tear trough and infraorbital hollow without compressing the deeper lymphatic structures.
Technique. A careful examination of the patient is made, being observant for any evidence of existing malar edema or malar bags. Inquiry about a history of cheek edema after excessive salt or alcohol intake or upon awakening is followed by a discussion to assure that the patient is in agreement with the treatment plan. In a patient who is unsure, a “trial run”, wherein lidocaine is injected to simulate her postinjection appearance, can be performed. Preinjection photographs are taken. Small volume, bilateral infraorbital nerve blocks are placed with 2% lidocaine (no more than 0.2mL). The filler is mixed with 2% lidocaine with 1:100,000 epinephrine.8 A volume of 0.2mL of 2% lidocaine with epinephrine is sterilely mixed with a 1.5mL syringe of CaHA and 0.08 of 2% lidocaine with epinephrine with a 0.8mL syringe of hyaluronic acid Juvederm Ultra (HA-JU, Allergan).
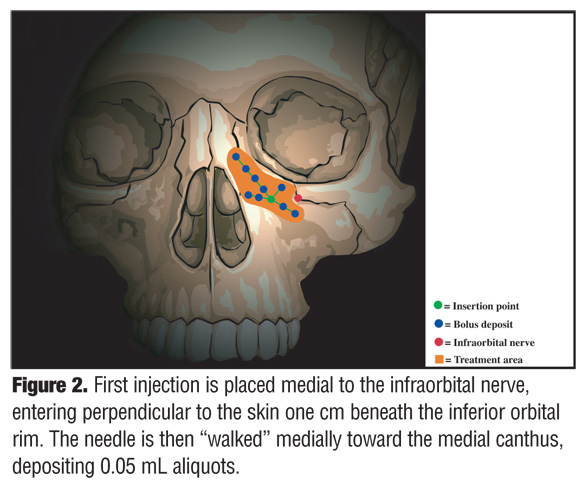
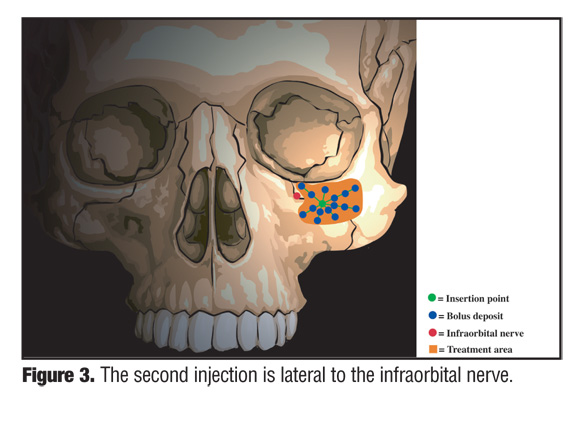
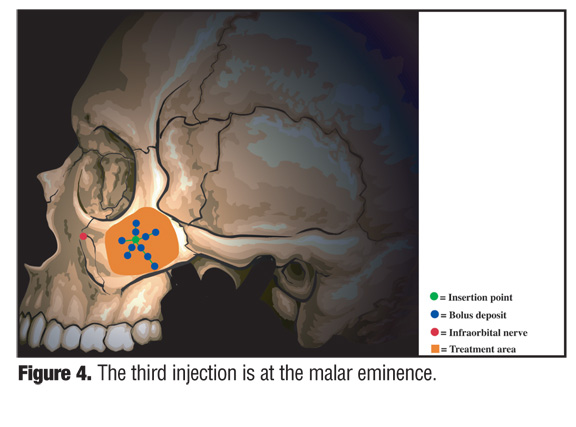
The first injection is placed medial to the infraorbital nerve, entering perpendicular to the skin approximately 1cm beneath the inferior orbital rim (Figure 2). The needle is then “walked” medially toward the medial canthus, depositing 0.05mL aliquots. Additional deposits are placed close to the orbital rim as well as laterally and inferiorly. The nondominant index finger is used to establish the inferior orbital rim location so as to prevent deposition of material into the orbital area. If the needle is in contact with the bone at the time of extrusion of filler, then the material will not be deposited into the infraorbital foramen or within the infraorbital nerve. The second injection is lateral to the infraorbital nerve; the third is at the malar eminence (Figure 3 and Figure 4).
{kind=link}
{kind=link}
{kind=link}
The final injection (not shown) is at the medial portion of the zygomatic arch. At each site, the needle is walked along the periosteum, depositing small amounts of filler without withdrawing the needle to limit the number of puncture sites and their resultant ecchymosis and edema. HA-JU is injected with a 30-gauge, 1/2-inch needle. CaHA is injected with a 28-gauge, 3/4-inch needle.
The material is molded to smoothness gently so as not to predispose the patient to ecchymoses. The purpose of molding is to smooth and manipulate the filler into the area of volume deficiency. Attention is directed when molding not to overly flatten or disperse the filler, necessitating higher volume of filler as a result of loss of correction. Overzealous massage can result in filler moving more superficially through needle tracts, thus increasing the propensity for visible material and malar edema. The ultimate objective is a smooth blending between the lower eyelid, nasolabial fold, and the cheek. All bleeding points are treated with immediate and sustained direct pressure. Postinjection ice packs and head elevation are employed.
Midfacial volume restoration using fillers is performed medially to laterally, since volumes should be most limited medially beneath the malar septum. Volumes need only be restricted by aesthetic goals when treating the malar eminence, lateral orbital rim, zygomatic arch, and submalar hollow. Facial volume restoration is performed correcting the midface prior to the lower face. Expansion of the midfacial soft tissue envelope will result in an effacement of the nasolabial folds and a reduction of the filler volume required for their correction.
Figure 5 and Figure 6 show three patients with malar edema who had been treated for volume enhancement using HA or CaHA, both injected through a transcutaneous approach using fanning and threading technique in the suborbicularis plane. In Figure 5, a 39-year-old female received HA into her tear troughs and infraorbital rims. She was treated with 20 units of Vitrase (ISTA Pharmaceuticals, Inc.) to ameliorate her malar edema. In Figure 6, a 44-year-old woman received a total of 1.3mL of CaHA in her midface (0.65mL per side), with malar edema evident five weeks post-treatment (A), and a 40-year-old woman received a total of 2.6mL of CaHA (1.3mL per side), with malar edema evident at three weeks post-treatment (B).
{kind=link}
{kind=link}
The author has performed more than 350 midfacial augmentations using this technique without any occurrence of malar edema or other significant adverse events, such as severe bruising, contour irregularities, visible material, or infraorbital nerve injury. The majority of patients were treated with a combination of CaHA and HA-JU. Average volume was one half a syringe of each material per side, i.e., 0.65mL of CaHA per side (in 1.3mL syringe) and 0.4mL of HA-JU per side. The HA-JU was injected in the area beneath the malar septum and the CaHA for enhancement of the malar eminence lateral to the lateral canthus. This approach was selected because of the ability to dissolve hyaluronic acid using hyaluronidase, if malar edema or other adverse event should occur. In addition, HA-JU has a significantly lower G’ than CaHA, making it less likely to compress the lymphatics of the area bounded by the malar septum. The higher G’, or lifting force exerted by CaHA, the more successfully elevated the thicker cheek tissues of the malar eminence, lateral orbital rim, and zygoma. Figure 7 is representative of the results obtained in the use of HA in the treatment of tear trough and infraorbital hollow.
{kind=link}
Recently, the author has employed the HA Belotero Basic (Merz), approved in Europe and recently approved in the United States, placed subcutaneously, for correction of tear troughs and infraorbital hollows, without adverse events. No Tyndall effect or visible material was observed. This HA was again combined with CaHA treatment of the malar eminence and inframalar hollow as aesthetically necessary.
Conclusion
Facial volume restoration and contour enhancement using dermal fillers have become a valuable addition to the aesthetic surgeon’s armamentarium. These techniques are relatively quick to perform, have little down time, and result in a high rate of patient satisfaction. Adverse events have been reported however, particularly when the area of the lower eyelid are injected. Although malar edema is a severe adverse event, its incidence can be reduced by proper patient selection, proper filler selection, limiting filler volume, and by placing filler material deep into the malar septum at the immediate preperiosteal level.
Acknowledgment
The author appreciates the editorial assistance of David J. Howell, PhD, RRT (San Francisco, California) in the development of this manuscript.
References
1. Tzikas TL. A 52-month summary of results using calcium hydroxylapatite for facial soft tissue augmentation. Dermatol Surg. 2008;34:S9–S15.
2. Graivier MH, Bass LS, Busso M, Jasin ME, Narins RS, Tzikas TL. Calcium hydroxylapatite (Radiesse) for correction of the mid- and lower face: consensus recommendations. Plast Reconstr Surg. 2007;120(Suppl):55S–66S.
3. Silvers SL, Eviatar JA, Echavez MI, Pappas AL. Prospective, open-label, 18-month trial of calcium hydroxylapatite (Radiesse) for facial soft-tissue augmentation in patients with human immunodeficiency virus-associated lipoatrophy: one-year durability. Plast Reconstr Surg. 2006;118(Suppl.): 34S–45S.
4. Werschler WP. Treating the aging face: a multidisciplinary approach with calcium hydroxylapatite and other fillers, part 2. Cosmetic Dermatol. 2007;20(12):791–796.
5. Busso M, Karlsberg PL. Cheek augmentation and rejuvenation using injectable calcium hydroxylapatite (Radiesse®). Cosmetic Dermatol. 2006;19:583–588.
6. Pessa JE, Garza JR. The malar septum: the anatomic basis of malar mounds and malar edema. Aesthetic Surg J. 1997;17(1):11–17.
7. Pessa JE, Zadoo VP, Adrian EK, Woodwards R, Garza JR. Anatomy of “black eye”: A newly described fascial system of the lower eyelid. Clin Anat. 1998;11:157–161.
8. Busso M, Voigts R. An investigation of changes in physical properties of injectable calcium hydroxylapatite in a carrier gel when mixed with lidocaine and with lidocaine/ epinephrine. Dermatol Surg. 2008;34:S16–S24.