
Joel L. Cohen, MD
Dr. Cohen is from the Department of Dermatology, University of Colorado, Denver; AboutSkin Dermatology and DermSurgery, Englewood, Colorado
The author reports no relevant conflicts of interest. Editorial support for this article, funded by Dermik Laboratories, a business of sanofi-aventis U.S. LLC, was provided by Albert Balkiewicz, MSc, of Peloton Advantage LLC. The author was fully responsible for the content, editorial decisions, and opinions expressed in the current article. The author received no honorarium or other form of financial support related to the development of this manuscript.
Abstract
Actinic keratosis is responsible for more than eight million visits to dermatologists and primary care physicians annually. Actinic keratosis, the result of chronic sun damage to the skin, is closely linked to nonmelanoma skin cancer, both histologically and pathophysiologically. Clinical evidence shows that not only does actinic keratosis have the potential to progress and transform into nonmelanoma skin cancer, but it also may in fact be an early stage of cancer. The treatment of actinic keratosis is evolving from a “treat-as-you-go” strategy to a more preventive approach to curtail the potential emergence of nonmelanoma skin cancer. As the interrelationship between actinic keratosis and nonmelanoma skin cancer, squamous cell carcinoma, and basal cell carcinoma continues to strengthen, treating actinic keratosis as part of a preventive strategy to reduce nonmelanoma skin cancer is coming to the forefront. The following review of the relationship between actinic keratosis and nonmelanoma skin cancer discusses the rationale for early actinic keratosis treatment to prevent or reduce nonmelanoma skin cancer occurrence. (J Clin Aesthetic Dermatol. 2010;3(6):39–44.)
Actinic keratosis (AK) is a common skin disease characterized by cutaneous lesions on the sun-exposed areas of fair-complected Caucasians.[1] AK prevalence in the United States and Australia has ranged from 11 to 26 percent in studies,1 and one study found that approximately 19 percent of Australians older than 40 years of age without a history of AK at study start developed one or more AKs within 12 months.[2]
AK was the primary diagnosis for 4.55 million visits to physicians from 1993 to 1994, according to the National Ambulatory Medical Care Survey,1 and comprised 14 percent of all US dermatologist visits over 10 years.[3] The annual frequency of AK visits stabilized from 1995 to 2003, but was predicted to increase as the population aged.[4] In fact, 2002 published data estimated that more than 8.2 million physician office visits were related to AK. This high AK prevalence translates into significant medical costs, with direct costs of AK surpassing one billion dollars annually.[5]
The clinical significance of AK relates to the risk of malignant transformation to nonmelanoma skin cancer (NMSC), including squamous cell carcinoma (SCC) and basal cell carcinoma (BCC). Although NMSC is treatable, some lesions, particularly SCC, may become locally invasive and destructive, potentially leading to metastasis or death. NMSC and its treatments may be associated with considerable morbidity, including functional impairments and cosmetic disfiguration, particularly from surgical procedures.[6]
The following article discusses the current clinical data surrounding the interrelationship between AK and NMSC, including clinical, histopathological, and genetic similarities. In addition, the evolving concept of treating AK as part of a strategy to prevent or reduce the risk of progression to malignant NMSC is reviewed.
Relationship Between AK and NMSC
NMSC, the most common skin malignancy, arises from epidermal keratinocytes. The majority of the one million new skin cancers diagnosed annually are NMSCs, with approximately 80 percent representing BCC and 16 percent representing SCC.[7] AK evolves from altered regulation of keratinocyte development and is most closely related to SCC among the NMSCs.[8,9]
AK and NMSC are interrelated; however, the nature and degree of this relationship remains controversial. Many investigators have suggested that an increased incidence of SCC exists within and around AK lesions. AK has been reported to be contiguous with SCC in 44,10 72,11 and 82 percent12 of cases.
Researchers have prospectively studied the rates of malignant transformation from AK to SCC. A five-year Australian study of 1,689 individuals seen for two consecutive years identified 21,905 AKs in the first examination year.13 The next year, 17 SCCs were identified as clearly arising from either an AK or normal skin. Of these 17 SCCs, 10 (59 percent) arose from an AK, and the other seven (41 percent) arose from clinically normal skin. The investigators calculated that the risk of an AK transforming to SCC within one year was less than 1 in 1,000.[13] Other investigators have reported much higher rates of malignant transformation. One study used a mathematical extrapolation to demonstrate that the 10-year risk of malignant transformation ranges from 6 to 10 percent.[14] In a retrospective medical records review of 6,691 patients with pathologically confirmed SCC, 91 patients (1.4%) had pathologically confirmed AK at the site of the subsequent SCC.[15]
Data from the VA Topical Tretinoin Chemoprevention (VATTC) trial provided insight on the potential for malignant progression of AK. After following 169 patients clinically and photographically for six years, rates of AK progression to SCC were calculated at 0.6 percent at one year and 2.6 percent at four years. Of these SCCs, 75 percent were considered invasive and the remainder were in situ.[16]
While similar topical formulations (e.g., 5-fluorouracil, imiquimod) treat AK and BCC, the progression of AK to BCC has not been critically accepted. However, recent studies have shown that AK may have a close relationship with or actually progress to BCC. The VATTC analysis showed the rate of AK progression to BCC as 0.5 percent at one year and 1.6 percent at four years, similar to those for AK progression to invasive SCC (0.4% at 1 year, 2.0% at 4 years).[16] A retrospective case review found the potential for AK or SCC in-situ lesions to overlie infiltrative or nodular BCC.[17] The area of AK/SCC conformed closely to the underlying BCC, and recognition of BCC was only achieved via deeper biopsy or during surgical consultation.
Clinical and Histologic Characteristics of AK and SCC
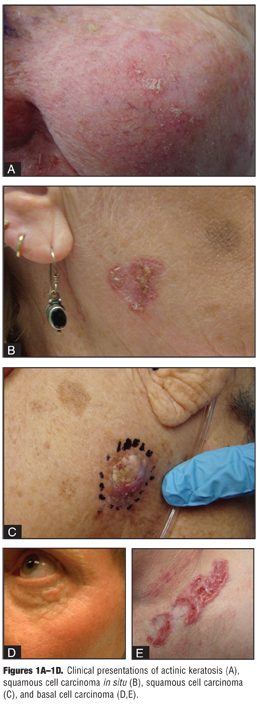
Clinical presentations of AK range from macular erythematous foci to large hyperkeratotic plaques. These lesions occur on sun-exposed areas, such as the head, neck, forearms, hands, and upper back.[9] Cutaneous SCC in situ occurs in a similar anatomic distribution, most typically as a fairly well-demarcated, hyperkeratotic, erythematous plaque.[9] Cutaneous SCC may be indurated or marked by firm papules, plaques, or nodules with hyperkeratosis, ulceration (well differentiated), or fleshy, soft, granulomatous papules or nodules without keratinization (poorly differentiated).[8,9] Some AKs become increasingly indurated and hyperkeratotic, which may complicate the clinical differentiation between AK and the more clinically serious SCC (Figures 1A–1D).[8,9]
{kind=link}
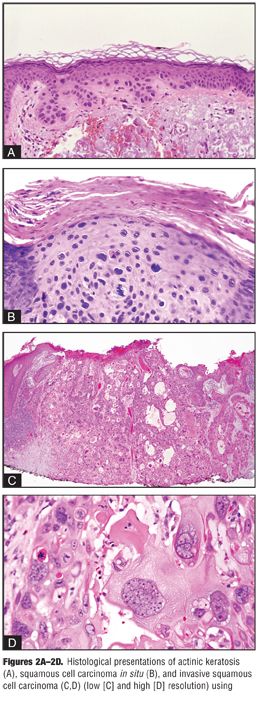
Histologically, AK is characterized by the presence of atypical keratinocytes in the deeper portions of the epidermis with defective maturation of the superficial epidermal layers, resulting in parakeratosis alternating with hyperkeratosis (Figure 2A).[9] Various histological subtypes have been described, including hypertrophic, atrophic, bowenoid, and acantholytic.[9] SCC is defined as atypical keratinocytes confined to the epidermis from the basal layer to the stratum corneum (in situ; Figure 2B
) or extension beyond the basement membrane into the dermis or deeper tissues (invasive; Figure 2C).[18]
{kind=link}
Preventive Strategies in AK and NMSC Management
The following key clinical points emerge when discussing AK and NMSC: 1) the risk of AK progression to SCC or BCC has been well documented, 2) a number of factors may predict the risk of AK progression to malignancy, and 3) the concept of AK as a form of SCC is becoming more accepted, but still critically debated. Predicting which AK will progress to NMSC is not possible; therefore, treating all AKs is essential to minimize the risk of NMSC.
Sequential and cumulative genetic damage are critical aspects of the pathogenesis of AK and NMSC. Primary prevention of ongoing ultraviolet-induced genetic damage is vital to reduce the development of AK and NMSC. As the genetic mechanisms involved in photodamage, cellular dysfunction, and deoxyribonucleic acid (DNA) repair become clearer, a shift in the management and treatment of NMSC is emerging. Preventive approaches for decreasing AKs and their associated risk of malignant transformation has gained attention. Based on the principle that AK and NMSC represent entities along a spectrum of clinically progressive disease, it follows that treatment of early clinical lesions (e.g., AK) or use of chemopreventive agents that modulate underlying molecular mechanisms may lower the incidence of invasive neoplasms and metastasis. Indeed, clinical medical societies have endorsed this principle by recommending early treatment of all AKs to reduce the potential for transformation and progression to NMSC.[19,20]
The Road to Chemoprevention in AK and NMSC Treatment
Chemoprevention represents the use of pharmacological interventions to potentially interrupt the development of new malignancies. Chemopreventive agents for skin cancer theoretically inhibit steps that occur after ultraviolet radiation exposure and before or during the development of tumor tissue. These strategies aim to treat the earliest signs of premalignant skin lesions, reducing the incidence of new lesions, recurrence of previous lesions, and progression to invasive and malignant disease.
Many therapies are available to manage AK, including destructive therapies (e.g., cryotherapy, surgical curettage), resurfacing techniques (e.g., dermabrasion, laser resurfacing, chemical peels), topical therapies (e.g., 5-fluorouracil, imiquimod, diclofenac gel, retinoids), and photodynamic therapy (PDT).[21] The efficacy of these treatments in reducing AK is well established and beyond the scope of this article; however, their prophylactic nature in preventing NMSC is less widely studied. The following review of clinical studies examines less common approaches to AK treatment and their effects on preventing NMSC over time.
Oral retinoids. Data on potential chemopreventive effects of oral retinoids (e.g., isotretinoin, etretinate, acitretin) are available. Retinoids help to maintain epithelial maturation and differentiation via their effects on growth factors, proto-oncogenes, and intracellular levels of ceramides.[22–24] The Southwest Skin Cancer Prevention Study Group studied 2,297 participants with a history of AK, SCC, or BCC who were randomly assigned for up to five years of daily dosing with 25,000IU oral retinol or placebo.22 The hazard ratio of first new SCC for the retinoid group was 0.74 (95% CI, 0.56–0.99; P=0.04), showing that they had a lower risk of developing new SCCs than the placebo group. The hazard ratio of first new BCC for the retinoid group was 1.06 (95% CI, 0.86–1.32; P=0.36), denoting that the risk of developing a new BCC was similar between the retinoid and placebo groups.[22] Similarly, a two-year course of high-dose oral isotretinoin was effective in the chemoprevention of SCC and BCC in five patients with xeroderma pigmentosa.24 The tumor frequency during the two-year treatment period was compared with an equivalent pretreatment interval, and the results indicated a 63-percent reduction in skin cancer (P=0.019). Interestingly, after discontinuing daily isotretinoin, the frequency of skin cancers in the posttreatment year was 8.5-fold higher than during the two-year treatment period (P=0.007).
Evidence indicates that oral retinoids may be helpful in the temporary chemoprevention of SCC; however, the likelihood of rebound must be carefully considered, as clinical evidence has demonstrated recurrence of SCC upon retinoid discontinuation.[25]
Photodynamic therapy. PDT is effective in treating AK and may have some chemotherapeutic properties. Methyl aminolevulinate (MAL) and illumination with broadband red light (75J/cm2, 570–670nm) was studied in 225 patients with SCC in situ. Lesion recurrence rates at 12 months after the last treatment were lower with MAL-PDT (15 percent) than with PDT-placebo (50 percent).[26] Similar benefits in reducing the development of BCC have been reported. PDT with 20-percent ALA and red light illumination in three children with BCC resulted in 85 to 98 percent overall clearance lasting up to six years.[27] This protection may have been due to destruction of subclinical lesions and/or induction of an antitumor response that suppresses development of new carcinomas. A randomized, split-face, placebo-controlled study examined the preventive effects of ALA-PDT with red light illumination in 45 patients with AK, extensive field cancerization on the face and scalp, and a history of previously diagnosed NMSC.[28] ALA-PDT significantly reduced new NMSC lesions over 12 months compared with placebo (14 vs. 30 total new NMSCs; P<0.001), but the prophylactic effect of PDT declined over time, with new lesion development increasing substantially six months after treatment.[28]
Additional chemopreventive approaches. Other treatments also may exert chemopreventive effects. In a five-year prospective trial, treatment with carbon dioxide laser, 30% trichloroacetic acid peel, or 5% 5-fluorouracil resulted in a reduction in AK of 83 to 92 percent (P=0.03), a lower incidence of NMSC than the control group (P=0.001), and a longer time to the development of new skin cancer than the control group (P=0.07). All three treatments were beneficial for AK reduction and skin cancer prophylaxis.[29]
Difluoromethylornithine, a chemopreventive agent, inhibits ornithine decarboxylase, an enzyme implicated in tumor promotion. In 48 patients with AK on the bilateral forearm, six-month difluoromethylornithine treatment reduced AKs by 23.5 percent (P=0.001) and significantly suppressed skin ornithine decarboxylase product levels (26 percent; P=0.04) compared with placebo.[30]
Other therapies postulated to possess chemopreventive potential in early investigational reports include topical thymidine dinucleotide[31] and liposomes containing T4 endonuclease.[32,33]
Chemoprevention and the Immunosuppressed Patient
In immunosuppressed patients (e.g., solid organ transplant patients), AK is a significant risk factor for SCC and BCC, more so than AK in immunocompetent individuals.[34] In a study of 915 solid-organ transplant recipients undergoing immunosuppressant therapy, AK was strongly associated with an increased risk of SCC, with adjusted odds ratios of 4.1 (1–49 AKs) and 12.1 (>50 AKs) compared with no lesions.[35] AKs were associated with BCC with adjusted odds ratios of 2.9 (1–49 AKs) and 4.0 (>50 AKs).
Immune surveillance is a key anticancer mechanism, as demonstrated by the 10- to 250-fold increased rates of AK, BCC, and SCC and the increased aggressiveness of disease in patients receiving immunosuppressants. Some immunosuppressants, such as azathioprine, may directly promote cancer formation, while agents such as cyclosporine have been implicated in the increased risk of SCC in this population.[34,36,37]
Chemopreventive strategies with possible utility in immunocompetent patients may not be as effective in immunosuppressed patients, possibly because the mechanisms of chemoprevention require an inherent immune response. Two studies assessed ALA-PDT (1–2 treatments) or MAL-PDT (two treatments) and 75J/cm[2] of visible light in treating AK and SCC in transplant versus immunocompetent patients.[38,39] Results showed clear persistence of residual disease, increased recurrence, and increased development of new lesions versus immunocompetent controls.[36,38,39] These data are supported by a study in organ transplant recipients in which two treatments with PDT utilizing d-ALA and violet light (400–450 nm) did not prevent formation of new SCC and had minimal effect on reducing AK after two years of follow up.40 In a study of PDT with broad-area ALA and a blue light PDT illuminator, 12 solid organ transplant recipients with multiple annual SCCs had all NMSC and other suspicious lesions removed and were treated with ALA-PDT up to nine times per year.[41] The average annual SCC count for each patient decreased from 18 at the baseline year to four in the first year of PDT and to one by the second year of PDT.
Persistent chemopreventive potential for some agents has been documented in immunocompromised patients. In a six-month randomized, double-blind, placebo-controlled trial of oral acitretin (30mg/day) in 44 renal transplant recipients with AK, the acitretin group had a significantly lower number of new NMSCs (P=0.01) and a lower total number of NMSCs (P=0.009) than placebo.[42] Of the patients with an established history of skin cancer, 1 of 9 in the treated group developed NMSC versus 7 of 10 in the placebo group (P=0.009). Similar effects were noted in renal transplant patients with oral etretinate, which is no longer available in the United States.[43] Based on these and other data, investigators concluded that oral retinoids have a role as chemopreventive agents against skin cancers in solid organ transplant recipients.[25,44,45]
Because of the potential adverse effects with long-term use of oral retinoids, topical approaches were postulated to be a more tolerable option in preventing AK and cutaneous malignancy as early as two decades ago.[46] Topical retinoids and topical 5-fluorouracil cream have been recommended for prophylactic use in organ transplant recipients with early (multiple AKs, isolated NMSC) or moderate (multiple cutaneous carcinomas per year) cutaneous carcinogenesis[34]; however, clinical evidence supporting topical retinoid use is nominal.
Conclusion
AK is a precursor to SCC and has been linked to potential BCC progression. The consensus is that AK may not be strictly distinct from SCC and that these two entities comprise a spectrum of histopathological abnormalities and clinical behaviors with ill-defined separation. Early treatment of AK has been recommended to reduce the potential for progression toward malignant disease. Clinical research on the progression of AK to NMSC supports the concept that treating AK may serve as a rational strategy for reducing the incidence of NMSC.
Although clinical data are limited on the long-term effects of common AK treatments and occurrence of NMSC, research examining the use of treatments, such as PDT, oral retinoids, 5-fluorouracil, and trichloroacetic acid peels, has shown potential benefit in terms of skin cancer prophylaxis and extending the time to NMSC occurrence in immunocompetent individuals. Similar, yet limited, results have been shown in immunocompromised patients as well with the use of acitretin, topical retinoids, and topical 5-fluorouracil. While no true chemopreventive approach exists to completely eliminate the occurrence of NMSC, reducing or prolonging the appearance of NMSC has been demonstrated via the successful treatment of AK. These data provide support for additional clinical studies examining the long-term effects of common AK treatments as a component of a chemopreventive strategy for reducing the occurrence of NMSC.
References
1. Salasche SJ. Epidemiology of actinic keratoses and squamous cell carcinoma. J Am Acad Dermatol. 2000;42(1 Pt 2):S4–S7.
2. Marks R, Foley P, Goodman G, et al. Spontaneous remission of solar keratoses: the case for conservative management. Br J Dermatol. 1986;115:649–655.
3. Gupta AK, Cooper EA, Feldman SR, Fleischer AB Jr. A survey of office visits for actinic keratosis as reported by NAMCS, 1990–1999. National Ambulatory Medical Care Survey. Cutis. 2002;70(2 Suppl):8–13.
4. Warino L, Tusa M, Camacho F, et al. Frequency and cost of actinic keratosis treatment. Dermatol Surg. 2006;32: 1045–1049.
5. The Lewin Group. The Burden of Skin Diseases: 2005. Falls Church, VA: The Lewin Group, for the Society for Investigative Dermatology and the American Academy of Dermatology Association; 2005.
6. Clayman GL, Lee JJ, Holsinger FC, et al. Mortality risk from squamous cell skin cancer. J Clin Oncol. 2005;23:759–765.
7. Einspahr JG, Stratton SP, Bowden GT, Alberts DS. Chemoprevention of human skin cancer. Crit Rev Oncol Hematol. 2002;41:269–285.
8. Alam M, Ratner D. Cutaneous squamous cell carcinoma. N Engl J Med. 2001;344:975–983.
9. Rossi R, Mori M, Lotti T. Actinic keratosis. Int J Dermatol. 2007;46:895–904.
10. Dinehart SM, Nelson-Adesokan P, Cockerell C, et al. Metastatic cutaneous squamous cell carcinoma derived from actinic keratosis. Cancer. 1997;79:920–923.
11. Czarnecki D, Meehan CJ, Bruce F, Culjak G. The majority of cutaneous squamous cell carcinomas arise in actinic keratoses. J Cutan Med Surg. 2002;6:207–209.
12. Mittelbronn MA, Mullins DL, Ramos-Caro FA, Flowers FP. Frequency of pre-existing actinic keratosis in cutaneous squamous cell carcinoma. Int J Dermatol. 1998;37:677–681.
13. Marks R, Rennie G, Selwood TS. Malignant transformation of solar keratoses to squamous cell carcinoma. Lancet. 1988;1:795–797.
14. Dodson JM, DeSpain J, Hewett JE, Clark DP. Malignant potential of actinic keratoses and the controversy over treatment. A patient-oriented perspective. Arch Dermatol. 1991;127:1029–1031.
15. Fuchs A, Marmur E. The kinetics of skin cancer: progression of actinic keratosis to squamous cell carcinoma. Dermatol Surg. 2007;33:1099–1101.
16. Criscione VD, Weinstock MA, Naylor MF, et al. Natural history and malignant progression of actinic keratoses: the VATTC trial [abstract 506]. J Invest Dermatol. 2008;128(Suppl 1):S85.
17. Sambandan PG, Goldman GD. Infiltrative basal cell carcinomas presenting as actinic keratosis: implications for clinical practice. Dermatol Surg. 2008;34:9–13.
18. Anwar J, Wrone DA, Kimyai-Asadi A, Alam M. The development of actinic keratosis into invasive squamous cell carcinoma: evidence and evolving classification schemes. Clin Dermatol. 2004;22:189–196.
19. Patients urged to seek treatment for actinic keratoses, recommends the American Academy of Dermatology, the American Cancer Society, and the Skin Cancer Foundation. Cutis. 1999;63:348.
20. Berman B, Bienstock L, Kuritzky L, et al. Actinic keratoses: sequelae and treatments. Recommendations from a consensus panel. J Fam Pract. 2006;55(Suppl):1–8.
21. Jorizzo JL, Carney PS, Ko WT, et al. Treatment options in the management of actinic keratosis. Cutis. 2004;74(6 Suppl):9–17.
22. Moon TE, Levine N, Cartmel B, et al. Effect of retinol in preventing squamous cell skin cancer in moderate-risk subjects: a randomized, double-blind, controlled trial. Southwest Skin Cancer Prevention Study Group. Cancer Epidemiol Biomarkers Prev. 1997;6:949–956.
23. Lebwohl M, Tannis C, Carrasco D. Acitretin suppression of squamous cell carcinoma: case report and literature review. J Dermatolog Treat. 2003;14(Suppl 2):3–6.
24. Kraemer KH, DiGiovanna JJ, Moshell AN, et al. Prevention of skin cancer in xeroderma pigmentosum with the use of oral isotretinoin. N Engl J Med. 1988;318:1633–1637.
25. Kovach BT, Sams HH, Stasko T. Systemic strategies for chemoprevention of skin cancers in transplant recipients. Clin Transplant. 2005;19:726–734.
26. Morton C, Horn M, Leman J, et al. Comparison of topical methyl aminolevulinate photodynamic therapy with cryotherapy or fluorouracil for treatment of squamous cell carcinoma in situ: results of a multicenter randomized trial. Arch Dermatol. 2006;142:729–735.
27. Oseroff AR, Shieh S, Frawley NP, et al. Treatment of diffuse basal cell carcinomas and basaloid follicular hamartomas in nevoid basal cell carcinoma syndrome by wide-area 5-aminolevulinic acid photodynamic therapy. Arch Dermatol. 2005;141:60–67.
28. Apalla Z, Sotiriou E, Chovarda E, et al. Skin cancer: preventive photodynamic therapy in patients with face and scalp cancerization. A randomized placebo-controlled study. Br J Dermatol. 2010;162:171–175.
29. Hantash BM, Stewart DB, Cooper ZA, et al. Facial resurfacing for nonmelanoma skin cancer prophylaxis. Arch Dermatol. 2006;142:976–982.
30. Alberts DS, Dorr RT, Einspahr JG, et al. Chemoprevention of human actinic keratoses by topical 2-(difluoromethyl)-dl-ornithine. Cancer Epidemiol Biomarkers Prev. 2000;9:1281–1286.
31. Arad S, Zattra E, Hebert J, et al. Topical thymidine dinucleotide treatment reduces development of ultraviolet-induced basal cell carcinoma in Ptch-1+/- mice. Am J Pathol. 2008;172:1248–1255.
32. Wolf P, Maier H, Mullegger RR, et al. Topical treatment with liposomes containing T4 endonuclease V protects human skin in vivo from ultraviolet-induced upregulation of interleukin-10 and tumor necrosis factor-alpha. J Invest Dermatol. 2000;114:149–156.
33. Yarosh D, Bucana C, Cox P, et al. Localization of liposomes containing a DNA repair enzyme in murine skin. J Invest Dermatol. 1994;103:461–468.
34. Berg D, Otley CC. Skin cancer in organ transplant recipients: epidemiology, pathogenesis, and management. J Am Acad Dermatol. 2002;47:1–17.
35. Bouwes Bavinck JN, Euvrard S, Naldi L, et al. Keratotic skin lesions and other risk factors are associated with skin cancer in organ-transplant recipients: a case-control study in The Netherlands, United Kingdom, Germany, France, and Italy. J Invest Dermatol. 2007;127:1647–1656.
36. Oseroff A. PDT as a cytotoxic agent and biological response modifier: implications for cancer prevention and treatment in immunosuppressed and immunocompetent patients. J Invest Dermatol. 2006;126:542–544.
37. Stockfleth E, Ulrich C, Meyer T, Christophers E. Epithelial malignancies in organ transplant patients: clinical presentation and new methods of treatment. Recent Results Cancer Res. 2002;160:251–258.
38. Dragieva G, Prinz BM, Hafner J, et al. A randomized controlled clinical trial of topical photodynamic therapy with methyl aminolaevulinate in the treatment of actinic keratoses in transplant recipients. Br J Dermatol. 2004;151:196–200.
39. Dragieva G, Hafner J, Dummer R, et al. Topical photodynamic therapy in the treatment of actinic keratoses and Bowen’s disease in transplant recipients. Transplantation. 2004;77:115–121.
40. de Graaf YG, Kennedy C, Wolterbeek R, et al. Photodynamic therapy does not prevent cutaneous squamous-cell carcinoma in organ-transplant recipients: results of a randomized-controlled trial. J Invest Dermatol. 2006;126:569–574.
41. Mehta S, Lee PK. ALA PDT for the chemoprevention of squamous cell carcinomas in chronically immunosuppressed solid organ transplant recipients at high risk of recurrence. Presented at: Combined Annual Meeting of the American Society of Dermatologic Surgery and American College of Mohs Micrographic Surgery and Cutaneous Oncology; October 27–30, 2005; Atlanta, GA.
42. Bavinck JN, Tieben LM, Van der Woude FJ, et al. Prevention of skin cancer and reduction of keratotic skin lesions during acitretin therapy in renal transplant recipients: a double-blind, placebo-controlled study. J Clin Oncol. 1995;13:1933–1938.
43. Gibson GE, O’Grady A, Kay EW, Murphy GM. Low-dose retinoid therapy for chemoprophylaxis of skin cancer in renal transplant recipients. J Eur Acad Dermatol Venereol. 1998;10:42–47.
44. Chen K, Craig JC, Shumack S. Oral retinoids for the prevention of skin cancers in solid organ transplant recipients: a systematic review of randomized controlled trials. Br J Dermatol. 2005;152:518–523.
45. Neuhaus IM, Tope WD. Practical retinoid chemoprophylaxis in solid organ transplant recipients. Dermatol Ther. 2005;18:28–33.
46. Peck GL. Topical tretinoin in actinic keratosis and basal cell carcinoma. J Am Acad Dermatol. 1986;15(4 Pt 2):829–835.