
James Q. Del Rosso, DO, Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada; Radhakrishnan Pillai, PhD, Associate Director Project Management, Dow Pharmaceutical Sciences Inc., Petaluma, California; Robert Moore, PhD, Associate Principal Scientist, Dow Pharmaceutical Sciences Inc., Petaluma, California
Disclosure: Dr. Del Rosso is a consultant, speaker, and researcher for Coria/Valeant, Allergan, Galderma, Graceway, Intendis, Medicis, Onset Therapeutics, Ortho Dermatologics, Pharmaderm/Nycomed, Promius, Ranbaxy, Stiefel/GSK, Triax, Unilever, and Warner-Chilcott. Drs. Pillai and Moore are employees of Dow Pharmaceutical Sciences Inc.
Abstract
Background: Clinicians have been reluctant to prescribe benzoyl peroxide concurrently with topical tretinoin due to a belief that the benzoyl peroxide may cause oxidation and degradation of the tretinoin molecule, thereby reducing its effectiveness. However, benzoyl peroxide-induced degradation of tretinoin may not necessarily apply to all topical tretinoin formulations. Objective: To evaluate the potential for benzoyl peroxide-induced degradation of an optimized aqueous gel formulation of tretinoin (0.05%). Methods: Tretinoin gel (0.05%) and benzoyl peroxide gel (6.26% premix concentration to produce 5% benzoyl peroxide in a fixed combination clindamycin product) were mixed together (1:1) at 32ºC and samples assayed after 1, 2, 3, 5, and 7 hours. Each sample was analyzed for tretinoin (expressed as % tretinoin remaining) and its degradation product content. Results: No loss of tretinoin was observed over the seven-hour time period. When tretinoin gel (0.05%) was combined with benzoyl peroxide, 100 percent of the initial tretinoin concentration remained after seven hours. There was no increase in the degradation products of tretinoin. Conclusions: There was no benzoyl peroxide-induced degradation of tretinoin when the optimized formulation of tretinoin gel (0.05%) was admixed with benzoyl peroxide gel (6.26%). Although the direct clinical significance of these results is unknown, clinicians may feel comfortable using this particular combination concurrently without concerns about tretinoin oxidation and degradation. (J Clin Aesthet Dermatol. 2010;3(10):26–28.)
Topical retinoids are one of the cornerstones of acne therapy and are recommended as a vital component of topical acne treatment. They may be used as monotherapy in mild comedonal acne. For inflammatory acne, topical retinoids are commonly used in combination with benzoyl peroxide (BPO) and antibiotics (topical or oral) and/or hormonal therapy in females.[1] However, when using topical combination therapy, the chemical compatibility and stability of the associated products needs to be taken into account, especially with concurrent or nearly concurrent timing of product application.
Tretinoin has been a commonly prescribed topical retinoid since its introduction in 1971 in the United States for acne treatment. Various concentrations and several formulations of tretinoin have been approved and introduced in the United States, each designed to reduce irritation and provide flexibility in dosing.[2] Clinicians have been reluctant to prescribe topical retinoids and BPO concurrently due to a belief that the BPO may result in oxidation and degradation of the tretinoin molecule, thereby reducing its effectiveness, and prefer to recommend the BPO or an antibiotic/BPO combination to be applied in the morning and tretinoin at night.[3] BPO is a strong oxidizer and the polyenic chains of tretinoin have been shown to be susceptible to oxidation.[3,4]
Most of the published data on degradation of tretinoin relates to photodegradation, although some data exists related to degradation by BPO of tretinoin when incorporated in certain vehicles. BPO lotion (10%) was shown to degrade tretinoin gel (0.025%) by 80 percent at 24 hours under inactinic light conditions, that is, irradiation without visible or ultraviolet wavelengths. However, when exposed to laboratory room light, the tretinoin content dropped rapidly.[5] The combination of BPO and light resulted in more than 50 percent degradation of tretinoin in two hours and 95 percent in 24 hours.[5] More recently, 89 percent of the tretinoin in tretinoin gel (0.025%) was shown to have undergone degradation after 24 hours of exposure to fluorescent light when it was combined with erythromycin-BPO topical gel.[6]
Case histories have demonstrated that clinically significant degradation of the retinoid molecule may not apply to all topical retinoid and BPO combinations.[7] New formulations of tretinoin are being developed that may protect the tretinoin from BPO-induced degradation and allow for more flexible dosing regimens. After eight hours of exposure, 94 to 95 percent of the initial tretinoin incorporated in a microsphere gel vehicle remained stable when combined with erythromycin-BPO topical gel and exposed to fluorescent light, incandescent light, or darkness, respectively, indicating about a five percent loss due to exposure to the BPO product even in the absence of light.[6] Another study with tretinoin gel microsphere 0.1% showed a 16 percent degradation in the presence of erythromycin/BPO or clindamycin/BPO after six hours of simulated solar ultraviolet irradiation.[8]
Degradation of tretinoin could potentially have an influence on both efficacy and adverse events, especially cutaneous tolerability. An optimized aqueous formulation of tretinoin gel (0.05%) has recently become available. Clinical studies have shown significantly (P<0.001) improved cutaneous tolerability over tretinoin gel microsphere (0.1%), but the potential for degradation of tretinoin with BPO of this optimized formulation of tretinoin gel (0.05%) has not been previously studied.[9]
METHODS
An in-vitro compatibility study was conducted using an optimized formulation of tretinoin gel (0.05%, Atralin® Gel, Coria Laboratories) and a 6.26% w/w BPO gel (the BPO gel which is combined with clindamycin to give a final concentration of BPO 5% w/w in a clindamycin-BPO combination product). Equal amounts of each gel were placed in an amber glass jar, mixed thoroughly, and duplicate 2g samples were removed. The jar was sealed with a polytetrafluoroethylene-lined cap and placed in a 32ºC water bath to simulate skin temperature. Each 2g sample was delivered into a 50mL volumetric flask and dissolved in 25mL of phosphate buffer (pH 3.0). Each flask was filled to volume with tetrahydrofuran. A portion of each sample solution was filtered through a 0.45µm polyvinylidene fluoride filter and assayed by high-performance liquid chromatography immediately after preparation. Additional duplicate samples were similarly prepared and analyzed after 1, 2, 3, 5, and 7 hours (see DPSI Standard Test Method 04-362, Revision 00 for the complete analytical procedure). Each sample was analyzed for tretinoin and degradation product content.
RESULTS
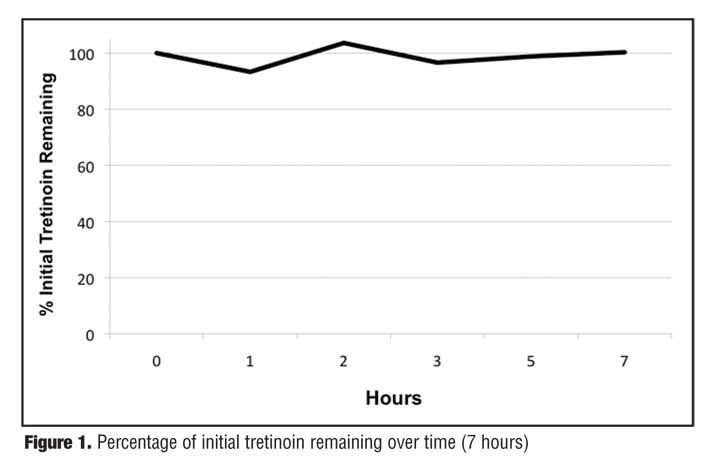
No loss of or decrease in tretinoin concentration was observed over the seven-hour time period ( Figure 1 ). The amount of tretinoin remaining after seven hours (100%) was unchanged from baseline.
{kind=link}
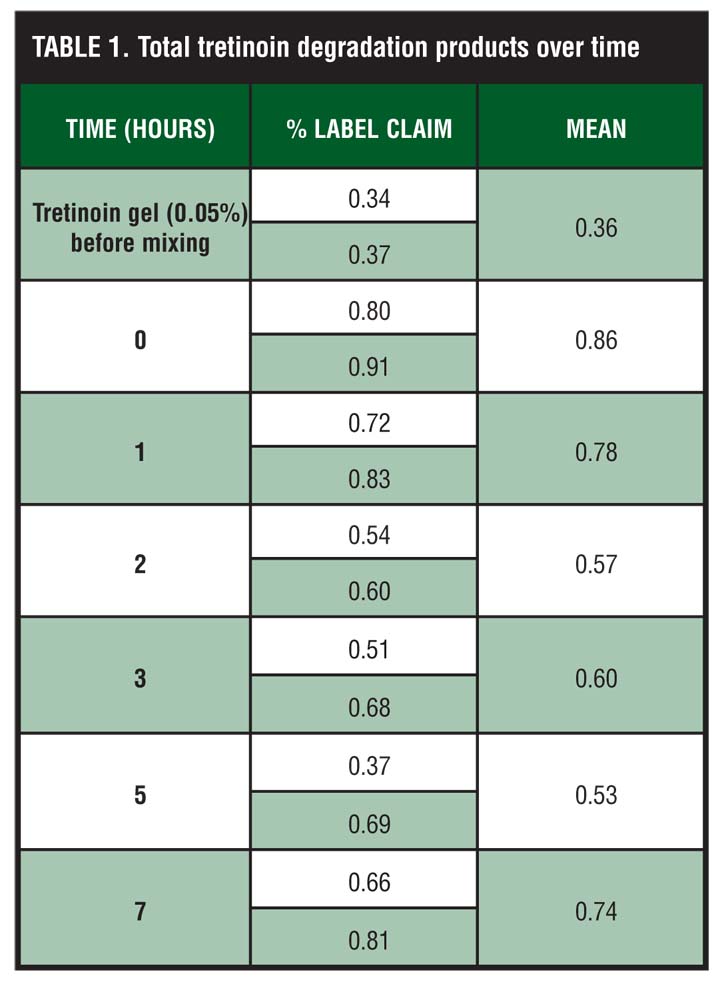
The total degradation product content is presented in Table 1. In addition to the degradation products observed in the tretinoin gel (0.05%)/BPO mixture, the total degradation products found in the tretinoin gel (0.05%) before mixing are reported. These values, 0.34% and 0.37% label claim, indicate the tretinoin gel (0.05%) used in this study has low levels of degradation prior to the addition of BPO gel. After mixing, the data shows an apparent initial increase in the total degradation product content, but no additional degradation over the seven-hour study period.
{kind=link}
DISCUSSION
It is important to appreciate that this is the worst-case scenario in terms of product mixing. Tretinoin and BPO are intimately mixed together and kept at 32ºC (to stimulate the temperature on the outer surface of skin). If patients with acne used these two products concurrently there would be less intimate contact between the two active products due to dilution on the skin surface with miscible components, such as sebum and cutaneous cells. The combination of an optimized formulation of tretinoin gel (0.05%) and BPO had no measurable effect on the amount of tretinoin in the mixture over seven hours. The low level of degradation products found confirms the lack of interaction between the two products when admixed as described above.
Combination therapy in acne is commonplace as multiple medications are used to target as many points in the pathogenesis of the disease as possible. Clinicians have been reluctant to prescribe BPO (either as monotherapy or in fixed combination with an antibiotic) concurrently with a topical retinoid, especially tretinoin, preferring to recommend the BPO or an antibiotic/BPO combination be applied in the morning and tretinoin at night. This is due to the widespread belief that applying topical tretinoin concurrently with a BPO-containing product may result in oxidation and degradation of the tretinoin molecule. Importantly, this information is based on a few studies that used a limited number of vehicles containing tretinoin, suggesting that this data may not necessarily be applicable to all formulations of tretinoin.[6]
In these fast-paced modern times, many people, including adolescents, have busy active lifestyles that should be considered when selecting appropriate acne treatment. Time of day and convenience of product application may affect whether a patient adheres to the treatment regimen. Morning applications may be inconvenient for adolescents or adults who have to rush off to work or school or for girls or women who have to wait for the product to absorb before applying makeup. The ability for a patient to apply the recommended topical therapies in a single “application session,” with the time of day determined by the patient, provides convenience that can often translate into better long-term adherence with therapy. This study suggests that using an optimized formulation of tretinoin gel (0.05%) concurrently with BPO will not diminish the efficacy of the tretinoin gel (0.05%) and should provide clinicians with more flexibility to tailor acne treatments to individual patient needs. Importantly, for the reasons explained above, the lack of BPO-induced degradation of tretinoin in this study may not apply to all topical tretinoin products and formulations.
ACKNOWLEDGMENT
The authors acknowledge the support of Brian Bulley, MSc, in the development of this manuscript.
References
1. Ghali F, Kang S, Leyden J, Shalita AR, Thiboutot DM. Changing the face of acne therapy. Cutis. 2009;83(2 Suppl):4–15.
2. Haider A, Shaw JC. Treatment of acne vulgaris. JAMA. 2004;292:726–735
3. Yan AC. Current concepts in acne management. Adolesc Med Clin. 2006;17(3):613–637.
4. Sporn, MB, Roberts AB, Goodman DS, eds. The Retinoids—Biology, Chemistry and Medicine. 2nd ed. New York: Raven Press; 1994.
5. Martin B, Meunier C, Montels D, Watts O. Brit J Dermatol. 1998;139(Suppl 52):8–11.
6. Nyirady J, Camelle L, Yusuf M, Migone P, Wisniewski S. The stability of tretinoin in tretinion gel microsphere 0.1%. Cutis. 2002;70:295–298.
7. Ditre CM. Case-based experience with the simultaneous use of a fixed topical antibiotic/benzoyl peroxide combination and a topical retinoid in the optimization of acne management. J Drugs Dermatol. 2009;8(12):1127–1131.
8. Nighland M, Yusuf M, Wisniewski S, et al. The effect of simulated solar UV irradiation on tretinoin in tretinoin gel microsphere 0.1% and tretinoin gel 0.025%. Cutis. 2006;77(5):313–316.
9. Webster G, Cargill I, Quiring J, Vogelson CT, Slade HB. A combined analysis of two randomized clinical studies of tretinoin gel 0.05% for the treatment of acne. Cutis. 2009, 83;146–154.